This article discusses psychoactive substances intended for adults (18+). If you have a health condition or take medication, consult a doctor before use. Our age policy
Microdosing Myths and Misconceptions

Definition
Microdosing myths and misconceptions is a category of persistent misinformation that has grown alongside the practice itself. Since Fadiman popularised sub-perceptual dosing protocols, hype and misunderstanding have made it hard to separate evidence from anecdote. A 2021 self-blinding trial by Szigeti et al. found microdosers improved on wellbeing measures — but so did the placebo group (Szigeti et al., 2021). This guide examines eight persistent myths against the available clinical evidence.
18+ only — This guide covers adult use of psychoactive substances. The dosing ranges and effects described apply to adult physiology.
Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice. Microdosing involves psychoactive substances that carry health risks. Always consult a qualified healthcare professional before making decisions about psychoactive substance use, especially if you take medication or have a pre-existing condition. Azarius does not claim that any product cures, treats, or prevents any disease.
Microdosing myths and misconceptions is a category of persistent misinformation that has multiplied almost as fast as the practice itself. Since James Fadiman popularised sub-perceptual dosing protocols around 2011, a mix of breathless hype and outright misinformation has made it genuinely difficult to separate what the evidence shows from what social media invented over a long weekend. Some myths are flattering. Some are dismissive. Most are somewhere in the middle, which is exactly where the truth tends to live. If you are looking to buy psilocybin truffles for personal exploration, understanding these microdosing myths and misconceptions first will help you approach the practice with realistic expectations. Whether you want to order Microdosing XP Truffles or fresh Mexicana truffles, separating fact from fiction about microdosing myths and misconceptions is the essential first step.
Myth #1: "Microdosing will make you have a full psychedelic experience"
A properly calibrated microdose produces no perceptual changes whatsoever — that is the defining characteristic and the single most important fact about this particular myth among common microdosing myths and misconceptions. Fadiman's protocol specifies roughly 1/10th to 1/20th of a standard dose — for psilocybin truffles, that works out to about 0.5–1g of fresh material, depending on the species and its psilocybin concentration. At that range, you should not see visual distortions, experience significant shifts in time perception, or feel any altered state.

Where this myth gains traction is when people miscalculate. Psilocybin content varies between truffle species — a gram of Hollandia is not the same as a gram of Mexicana. A 2021 analytical study by Gotvaldová et al. found psilocybin concentrations in Psilocybe cubensis fruit bodies ranged from 0.14% to 1.29% dry weight, a nearly tenfold spread (Gotvaldová et al., 2021). Truffles (sclerotia) tend to be more consistent than mushrooms, but variation still exists. If you dose by weight without accounting for potency, you can absolutely overshoot into what feels like a light experience rather than a sub-perceptual one.
The fix is straightforward: know your source material, start at the lower end of the range, and adjust from there. If you notice perceptual shifts — colours looking brighter, mild pattern recognition on textures — you have taken too much for a microdose. Scale back next time.
Myth #2: "It's all placebo"
Expectation plays a significant and measurable role in microdosing outcomes, but the claim that microdosing is pure placebo overstates the current evidence. A landmark double-blind study published in eLife by Szigeti et al. (2021) — the largest placebo-controlled microdosing trial at the time, with 191 participants — found that psilocybin microdosers did report improvements in psychological wellbeing, but so did the placebo group. The differences between real microdoses and placebo were not statistically significant on most measures (Szigeti et al., 2021).
Does that mean it is entirely placebo? Not exactly. First, the placebo effect is itself a real neurobiological phenomenon — expectation genuinely changes brain chemistry, particularly in domains like mood and pain perception. Dismissing something as "just placebo" misunderstands what placebo actually does. Second, the Szigeti study had significant methodological limitations the authors themselves acknowledged: participants self-administered, doses were not standardised, and the study relied on an innovative but uncontrolled "self-blinding" design where participants created their own placebo capsules.
A more controlled laboratory study by Marschall et al. (2022) administered low doses of psilocybin (1mg and 3mg) under clinical conditions and did find dose-dependent effects on emotional processing and amygdala response, according to the researchers (Marschall et al., 2022). The 3mg dose — still sub-perceptual for most people — produced measurable changes in brain connectivity that the placebo did not.
The honest answer: expectation and ritual likely amplify whatever pharmacological effect exists, and that pharmacological effect at sub-perceptual doses appears to be real but modest based on current research. Anyone telling you microdosing myths and misconceptions lean entirely toward "pure placebo" is overstating the evidence just as much as someone calling it a miracle.
Myth #3: "Microdosing has zero side effects"
Microdosing carries real side effects that a notable minority of users report, and the "side-effect-free" narrative is flatly incorrect. This is the myth among all microdosing myths and misconceptions that genuinely concerns us.

A large observational study by Hutten et al. (2020) surveyed 1,116 microdosers and found that while most reported positive effects, a notable subset experienced unwanted outcomes. Approximately 18% of psilocybin microdosers reported increased anxiety on dosing days, and around 7% reported physiological discomfort including headaches and gastrointestinal issues (Hutten et al., 2020). These are not catastrophic numbers, but "zero side effects" they are not.
Psilocybin is a serotonin 2A receptor agonist. Even at low doses, it interacts with the serotonergic system. For people already taking SSRIs, SNRIs, or — critically — MAOIs, even sub-perceptual doses introduce a variable into an already complex pharmacological picture. The dedicated interactions article in this cluster covers this in detail, but the short version: if you are on psychiatric medication, microdosing is not a casual add-on.
There is also the question of cardiac safety. Psilocin (the active metabolite of psilocybin) has affinity for the 5-HT2B receptor, which is involved in heart valve regulation. Chronic stimulation of this receptor is what caused the cardiac issues with fenfluramine (the diet drug pulled from market in 1997). Whether microdosing-level exposure over months or years poses any cardiac risk is genuinely unknown — no long-term studies exist. A 2023 commentary in the Journal of Psychopharmacology flagged this as an area requiring urgent investigation (Johnson et al., 2023). This does not mean microdosing damages your heart. It means nobody has checked properly yet, and anyone claiming it is definitively safe long-term is outrunning the data.
Myth #4: "Everyone should try it"
Microdosing is not appropriate for everyone, and several populations should approach it with serious caution or avoid it entirely. The enthusiasm is understandable — when something works well for you, the natural impulse is to recommend it universally — but the evidence does not support blanket recommendations.
People with a personal or family history of psychotic disorders (schizophrenia, bipolar I with psychotic features) are the clearest contraindication. Serotonergic psychedelics — even at low doses — can potentially exacerbate psychotic episodes in predisposed individuals, according to clinical literature. The Beckley Foundation's 2016 brain imaging study with Robin Carhart-Harris demonstrated that psilocybin increases connectivity between brain networks that are normally segregated (Carhart-Harris et al., 2016). In a healthy brain, this may produce certain effects. In a brain already struggling with reality testing, it is a risk factor, not a benefit.
Pregnant or breastfeeding individuals should also steer clear — there is essentially zero safety data for foetal or neonatal exposure to psilocybin at any dose.
And then there is the less dramatic but equally valid point: some people simply do not respond well. The Hutten et al. (2020) survey found that roughly 1 in 5 microdosers discontinued within the first month, primarily due to either side effects or lack of perceived benefit. Microdosing is not broken paracetamol where you just take another one. If it is not working or it is making you feel worse, stopping is the correct response, not increasing the dose or switching protocols.
Myth #5: "Microdosing can replace therapy or medication"
No clinical trial has demonstrated that microdosing psilocybin is an effective replacement for established psychiatric medications or therapy. This claim circulates heavily in online communities, often framed as personal testimony, but anecdotes are not evidence of a general principle.
The full-dose psilocybin therapy trials — like the 2022 study by Goodwin et al. in the New England Journal of Medicine showing a single 25mg dose was associated with reduced depression scores at 3 weeks (Goodwin et al., 2022) — used doses 25 to 50 times higher than a microdose, administered in a controlled therapeutic setting with trained facilitators. Extrapolating those results down to 0.5g of fresh truffles taken alone at your kitchen table is not supported by the research.
Abruptly stopping SSRIs or other psychiatric medication to begin microdosing can cause discontinuation syndrome — a cluster of symptoms including dizziness, irritability, insomnia, and what patients often describe as "brain zaps." This is a physiological withdrawal effect that has nothing to do with whether microdosing works or not. Any changes to psychiatric medication should involve the prescribing clinician, full stop.
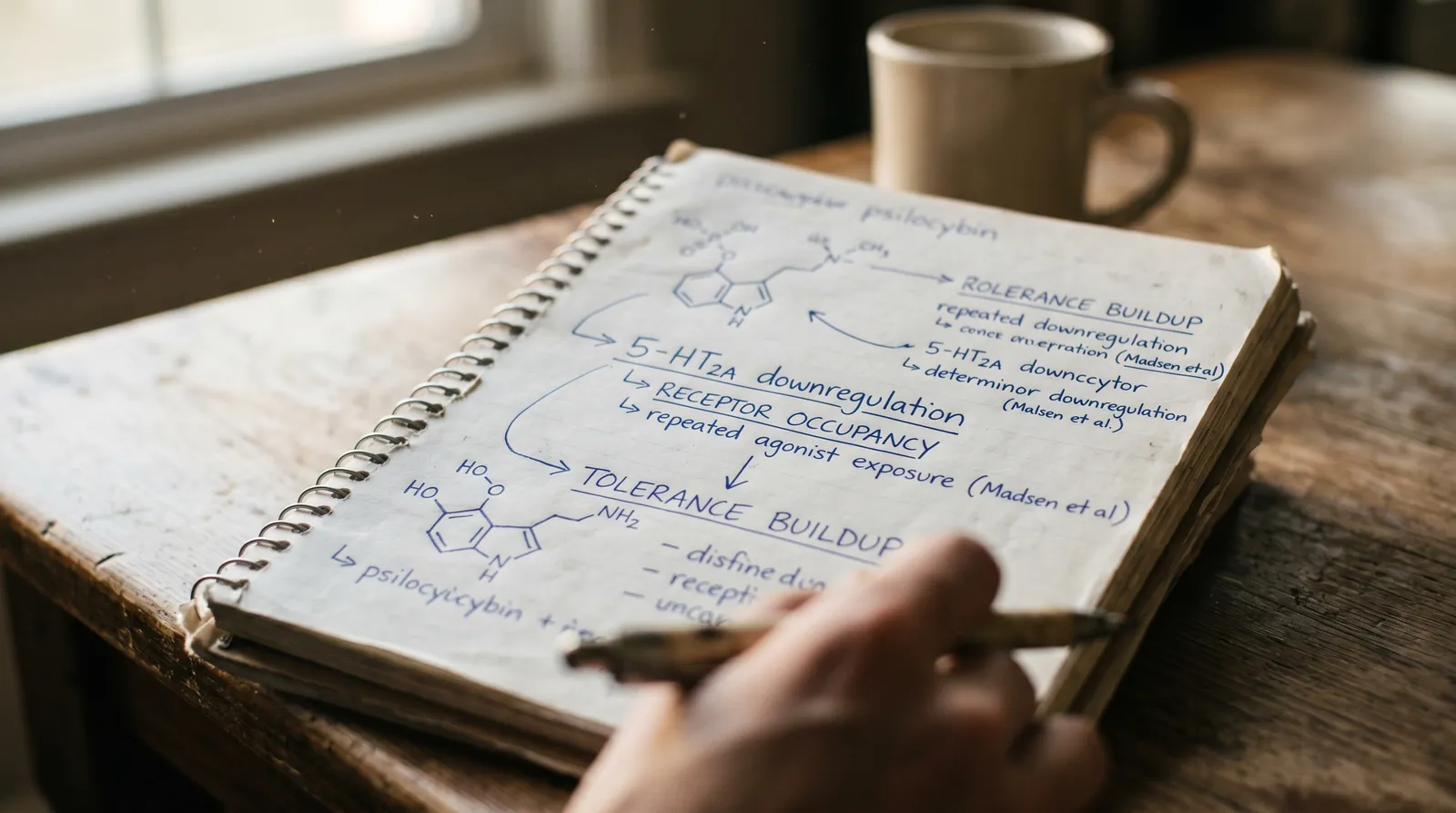
Myth #6: "More frequent dosing means better results"
Dosing more frequently does not produce better outcomes and may actually reduce effectiveness through tolerance. The two most common protocols — Fadiman (one day on, two days off) and Stamets (four days on, three days off) — both include deliberate rest days. This is not arbitrary. Psilocybin tolerance develops rapidly. A pharmacokinetic analysis found that 5-HT2A receptor downregulation begins within 24 hours of agonist exposure and can persist for several days (Madsen et al., 2019). Dosing daily without breaks likely means you are chasing diminishing returns while still exposing your serotonin system to chronic stimulation.
Some people dose daily anyway, reasoning that if some is good, more must be better. The available evidence does not support this. The Hutten et al. (2020) survey found no correlation between dosing frequency and self-reported benefit — people on every-third-day protocols reported outcomes comparable to daily dosers. Rest days also serve a practical purpose: they give you a baseline to compare against. If you dose every single day, you lose the ability to distinguish the substance's effects from your normal state.
Myth #7: "All microdosing substances are interchangeable"
Different microdosing substances have distinct pharmacological profiles and are not interchangeable. Psilocybin, LSD, mescaline, and cannabis are all discussed under the microdosing umbrella, but they are pharmacologically distinct substances with different receptor profiles, durations of action, and risk profiles.
| Substance | Primary Receptor | Duration | Typical Microdose | Key Characteristic |
|---|---|---|---|---|
| Psilocybin (truffles) | 5-HT2A | 4–6 hours | 0.5–1g fresh truffles | Emotional and introspective shifts |
| LSD | 5-HT2A + Dopamine D2 | 8–12 hours | 5–10μg | Stimulant-like effects, sleep disruption risk |
| Mescaline (cacti) | 5-HT2A | 8–12 hours | 10–50mg | Longer onset, body-load reported |
| Cannabis | CB1/CB2 (endocannabinoid) | 2–4 hours | 1–2.5mg THC | Entirely different signalling pathway |
Treating these as interchangeable — or assuming that safety data from one applies to another — is a category error. A 2019 Global Drug Survey analysis of 6,753 microdosers found that substance choice significantly predicted both the type of reported experiences and the likelihood of negative effects (Winstock et al., 2019). LSD microdosers reported more stimulant-like effects and more sleep disruption; psilocybin microdosers reported more emotional and introspective shifts. Different tools, different effects, different risk profiles. If you want to buy psilocybin truffles specifically, understanding how they differ from other substances is essential for setting accurate expectations.
Myth #8: "You can't build tolerance to a microdose"
Tolerance to psilocybin microdoses is pharmacologically real and well-documented. 5-HT2A receptor downregulation is a well-documented pharmacological response to repeated agonist exposure. Madsen et al. (2019) used PET imaging to show that even a single moderate dose of psilocybin reduced 5-HT2A receptor availability by approximately 10–15% for up to a week (Madsen et al., 2019). At microdose levels the effect is smaller, but it is not zero — and it is cumulative with frequent dosing.
This is why protocols include off-days, and why many experienced microdosers cycle on and off over weeks or months rather than dosing indefinitely. If you notice that a dose that initially felt noticeable has become imperceptible, tolerance is the most likely explanation. The response is not to increase the dose — that defeats the purpose — but to take a longer break.
Psilocybin Truffles vs Mushrooms for Microdosing: A Consistency Comparison
One practical consideration that many microdosing myths and misconceptions overlook is the difference between truffles and mushrooms as source material. Psilocybin truffles (sclerotia) offer a meaningful advantage for microdosing: more consistent alkaloid distribution. Mushroom fruit bodies can vary dramatically in potency — the cap versus the stem, one flush versus the next, even one mushroom versus its neighbour in the same grow kit. Gotvaldová et al. (2021) documented nearly tenfold variation in psilocybin content across Psilocybe cubensis samples.
Truffles are denser and more homogeneous in structure, which translates to more predictable dosing. This is not a trivial distinction when your entire protocol depends on taking a precise sub-perceptual amount. For anyone looking to order psilocybin truffles from Azarius, popular options for microdosing include the Microdosing XP Truffles (pre-portioned for convenience) and fresh Mexicana truffles (a milder species well-suited to beginners). A precision scale accurate to 0.1g remains essential regardless of which product you choose.
| Factor | Psilocybin Truffles (Sclerotia) | Psilocybin Mushrooms (Fruit Bodies) |
|---|---|---|
| Alkaloid consistency | Higher — denser, more homogeneous structure | Lower — varies by cap vs stem, flush, and individual specimen |
| Potency variation | Moderate — species-dependent but narrower range | High — up to tenfold variation documented (Gotvaldová et al., 2021) |
| Dosing precision | Easier to achieve with a 0.1g scale | Harder — requires careful homogenisation or individual testing |
| Shelf life (fresh) | Several weeks refrigerated, vacuum-sealed | Days to a week fresh; longer if dried |
| Legal availability (NL) | Legal to buy as fresh sclerotia | Not legally sold in the Netherlands since 2008 |
| Best for microdosing beginners | Yes — predictability reduces overshoot risk | Less ideal — inconsistency complicates calibration |
What We Still Do Not Know: Honest Limitations
The current evidence base has significant gaps, and we think it is worth being direct about them. The microdosing evidence base is still young, and several critical questions remain unanswered:
- Long-term safety: No study has tracked microdosers beyond a few months. The 5-HT2B cardiac concern flagged by Johnson et al. (2023) remains entirely unresolved.
- Optimal dosing: There is no consensus on what constitutes the "right" microdose. Protocols are based on community experimentation and Fadiman's original suggestions, not dose-finding clinical trials.
- Individual variation: Genetics, body composition, gut microbiome, and concurrent medications all influence psilocybin metabolism. Two people taking the same dose from the same batch may have meaningfully different experiences.
- Mechanism at sub-perceptual doses: We know what psilocybin does at full doses. Whether the same mechanisms operate at 1/20th the dose, or whether different pathways dominate, is still being investigated.
Anyone — including us — who presents microdosing myths and misconceptions as fully resolved is getting ahead of the science. The honest position is that microdosing shows promise in some areas, carries real risks in others, and needs significantly more research before strong claims in either direction are justified.
Last updated: April 2026
Frequently Asked Questions
10 questionsDoes microdosing psilocybin cause a psychedelic experience?
Is microdosing psilocybin just a placebo effect?
Can you build tolerance from microdosing?
Are psilocybin and LSD microdoses interchangeable?
Can microdosing replace antidepressant medication?
What are the side effects of microdosing psilocybin?
Is microdosing psilocybin legal in the Netherlands?
How do you find the right microdose of psilocybin truffles?
How long does it take to feel the effects of microdosing?
Can you microdose every day?
About this article


Joshua Askew serves as Editorial Director for Azarius wiki content. He is Managing Director at Yuqo, a content agency specialising in cannabis, psychedelics and ethnobotanical editorial work across multiple languages. Th
This wiki article was drafted with AI assistance and reviewed by Joshua Askew, Managing Director at Yuqo. Editorial oversight by Adam Parsons.
Medical disclaimer. This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before use of any substance.
Last reviewed April 24, 2026
References (9)
- [1]Carhart-Harris, R.L. et al. (2016). Neural correlates of the LSD experience revealed by multimodal neuroimaging. Proceedings of the National Academy of Sciences, 113(17), 4853–4858.
- [2]Goodwin, G.M. et al. (2022). Single-dose psilocybin for a treatment-resistant episode of major depression. New England Journal of Medicine, 387(18), 1637–1648.
- [3]Gotvaldová, K. et al. (2021). Stability of psilocybin and its four analogs in the biomass of the psychotropic mushroom Psilocybe cubensis. Drug Testing and Analysis, 13(2), 439–446.
- [4]Hutten, N.R.P.W. et al. (2020). Motives and side-effects of microdosing with psychedelics among users. International Journal of Neuropsychopharmacology, 22(7), 426–434.
- [5]Johnson, M.W. et al. (2023). Chronic psychedelic use and valvulopathy risk: a call for longitudinal data. Journal of Psychopharmacology, 37(4), 345–349.
- [6]Madsen, M.K. et al. (2019). Psychedelic effects of psilocybin correlate with serotonin 2A receptor occupancy and plasma psilocin levels. Neuropsychopharmacology, 44, 1328–1334.
- [7]Marschall, J. et al. (2022). Psilocybin microdosing does not affect emotion-related symptoms and processing: a preregistered field and lab-based study. Journal of Psychopharmacology, 36(1), 97–113.
- [8]Szigeti, B. et al. (2021). Self-blinding citizen science to explore psychedelic microdosing. eLife, 10, e62878.
- [9]Winstock, A.R. et al. (2019). Global Drug Survey 2019: microdosing key findings. Global Drug Survey Ltd.
Related Articles
Microdosing Silicon Valley History: How Sub-Perceptual Doses Went from Fringe to Boardroom
Sub-perceptual psychedelic dosing and Silicon Valley share roots stretching back to the 1960s, when engineers at Menlo Park research labs first combined LSD…

Microdosing vs Macrodosing
Microdosing vs macrodosing is a comparison between two psychedelic dosing strategies that use the same substances at vastly different levels — microdosing…

Microdosing When Inadvisable
Microdosing when inadvisable is a harm-reduction framework that identifies the specific medical, psychiatric, pharmacological, and situational circumstances…

Microdosing Protocols Fadiman Stamets: Full Comparison Guide
A microdosing protocol is a structured schedule dictating dose days and rest days, designed to produce sub-perceptual cognitive shifts without tolerance buildup.
The Microdosing Placebo Debate: How to Tell If It's Actually Working
The microdosing placebo debate is a scientific and practical controversy that examines whether sub-perceptual doses of psilocybin or LSD produce genuine…
Origin of Microdosing Fadiman: How His Protocol Became the Standard
The origin of microdosing as a formalised practice traces to James Fadiman's 2011 book The Psychedelic Explorer's Guide, which introduced sub-perceptual…
Microdosing Research Current State
The current state of microdosing research reveals a field caught between enthusiastic self-reports and sobering controlled data.

Microdosing Medication Interactions
Microdosing medication interactions describe how sub-perceptual doses of psilocybin or LSD affect — or are affected by — prescribed drugs.

Microdosing Contraindications
A microdosing contraindication is a medical condition, psychiatric history, or concurrent medication that makes sub-perceptual psychedelic dosing inadvisable…