This article discusses psychoactive substances intended for adults (18+). If you have a health condition or take medication, consult a doctor before use. Our age policy
Microdosing Harm Reduction Principles
Definition
Microdosing harm reduction is a structured set of practical guidelines that keeps sub-perceptual dosing of psychoactive substances safe and intentional. Kuypers et al. (2019) found that self-reported benefits outpaced challenges only when participants followed structured protocols with deliberate rest days. These principles cover dose accuracy, protocol selection, contraindication screening, and knowing when to stop.
18+ only — this guide is written for adults. The dosing ranges, protocols, and physiological considerations below apply to adult bodies and adult decision-making.
Microdosing harm reduction is a structured set of practical guidelines that keeps sub-perceptual dosing of psychoactive substances — most commonly psilocybin truffles or LSD — as physically and psychologically safe as possible. A 2019 systematic review by Kuypers et al. found that while microdosing research is still in its early stages, self-reported benefits consistently outpaced self-reported challenges — but only when participants followed structured protocols with deliberate rest days (Kuypers et al., 2019). The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) has noted the growing prevalence of microdosing practices across Europe, underscoring the need for evidence-based harm reduction guidance. The steps below aren't abstract theory. They're the distilled version of what actually keeps people out of trouble.
Step 1: Know Your Substance and Its Dose Range
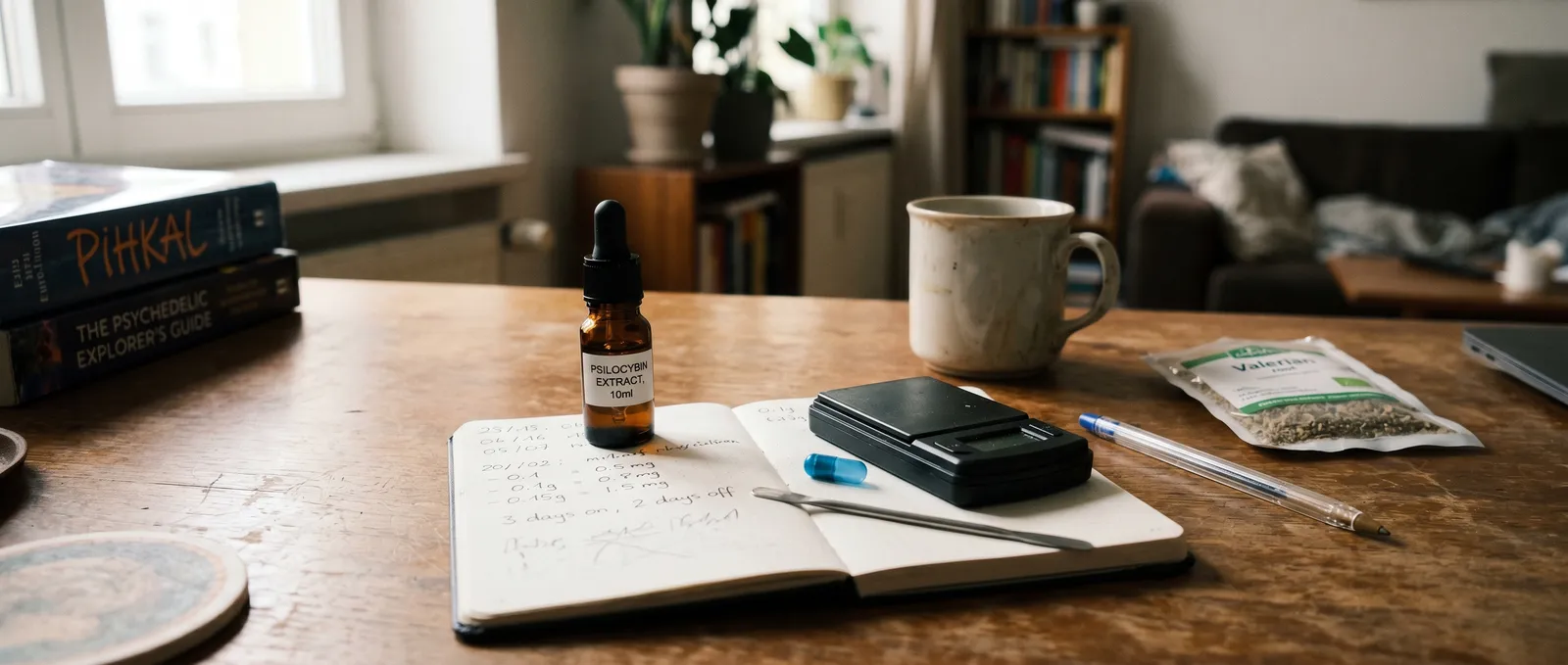
The correct dose range is the single most important variable in microdosing harm reduction. "Microdose" is not a feeling — it's a dose range, and it differs by substance. For psilocybin (whether from truffles or dried mushrooms), research protocols have typically used between 0.5 g and 1.5 g of fresh truffles, or roughly 0.1–0.3 g of dried Psilocybe cubensis fruit bodies. For LSD, studies have used 5–20 µg — a fraction of a full dose of 100–200 µg (Hutten et al., 2019).

The critical distinction: a microdose should be sub-perceptual. You should not feel altered. If colours look brighter, if music sounds different, if you're getting tracers in your peripheral vision — that's not a microdose, that's a low dose, and the microdosing harm reduction calculus changes entirely. A genuine microdose lets you go about your day without anyone (including you) noticing anything dramatic.
Potency varies between batches, strains, and individual truffles. A 1 g portion of one truffle variety can contain meaningfully different psilocybin concentrations than 1 g of another. Weighing with a scale accurate to 0.01 g is not optional — it's the single most effective harm reduction tool you own. If you want to buy a precision scale, get one that reads to 0.01 g; anything less precise is not fit for purpose.
Step 2: Choose a Protocol and Stick to It
A structured dosing schedule is the most reliable way to prevent tolerance build-up and psychological dependence. Protocols exist to prevent two problems: tolerance build-up and psychological dependence on a daily ritual. The two most referenced schedules in the literature and community are:
| Protocol | Schedule | Origin | Rest Days per Week |
|---|---|---|---|
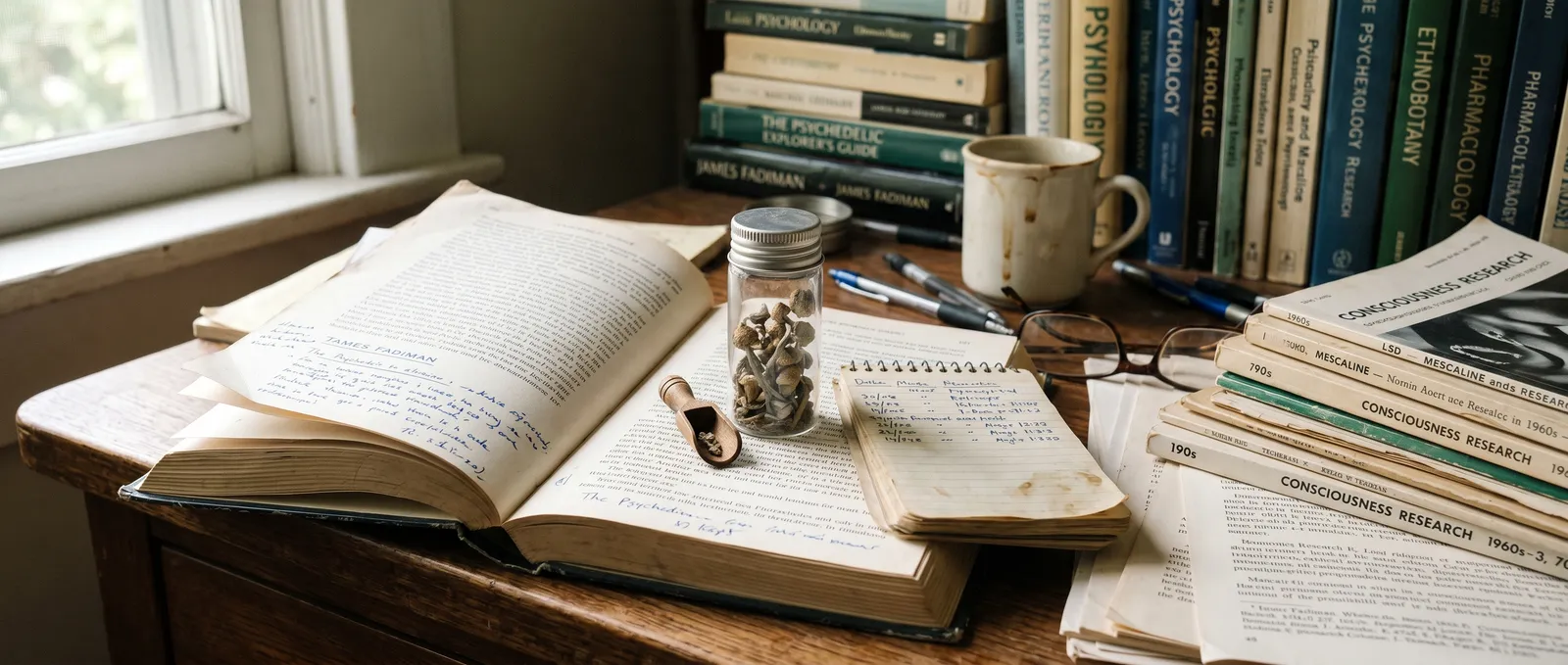
| Fadiman Protocol | Day 1: dose, Day 2: off, Day 3: off, repeat | James Fadiman's self-blinding research (2011) | 4–5 |
| Stamets Stack | 4 days on, 3 days off | Paul Stamets (combined with lion's mane and niacin) | 3 |
| Every-other-day | Dose, off, dose, off | Community-derived | 3–4 |
| Intuitive | Dose when "it feels right" | No formal origin | Varies — often too few |
The "intuitive" approach is the one that most often goes sideways. Without built-in rest days, serotonin receptor down-regulation (tolerance) creeps in within 7–10 days, and you end up increasing the dose to chase the same subtle effect — which is exactly the opposite of microdosing harm reduction. Pick a structured protocol. Write it on a calendar. Treat rest days as non-negotiable.
Most protocols suggest running for 4–8 weeks, then taking at least 2–4 weeks off entirely. This isn't arbitrary caution: a 2022 placebo-controlled study from Imperial College London found that expectation effects accounted for a significant portion of self-reported microdosing benefits, and periodic breaks help you distinguish between pharmacological effects and placebo (Szigeti et al., 2022). The break is where you find out what the substance is actually doing versus what you believe it's doing.
Fadiman vs. Stamets: Which Protocol Fits?
The Fadiman protocol gives you more rest days and is simpler to follow — dose once, take two days off, repeat. It's the better starting point if you've never microdosed before. The Stamets Stack adds lion's mane mushroom and niacin (vitamin B3) to the psilocybin dose, with four consecutive dose days followed by three off. The idea is that lion's mane supports neurogenesis while niacin drives peripheral vasodilation, theoretically improving distribution. Honestly, the evidence for this specific combination is almost entirely anecdotal — no controlled trial has tested the Stamets Stack as a unit. We've seen customers order both lion's mane capsules and microdosing truffles together, and the ones who track their results carefully tend to prefer the Fadiman schedule for its simplicity and clearer signal-to-noise ratio.
Step 3: Control Your Variables
Variable control is what separates useful self-experimentation from guesswork. Harm reduction isn't only about the substance. It's about everything around it.
Timing. Take your microdose in the morning, ideally before noon. Even sub-perceptual amounts of psilocybin can affect sleep architecture if taken late in the day. A 2021 survey of 1,116 microdosers by Rootman et al. found that roughly 18% reported sleep disruption as a negative effect — and most of those dosed in the afternoon or evening (Rootman et al., 2021).
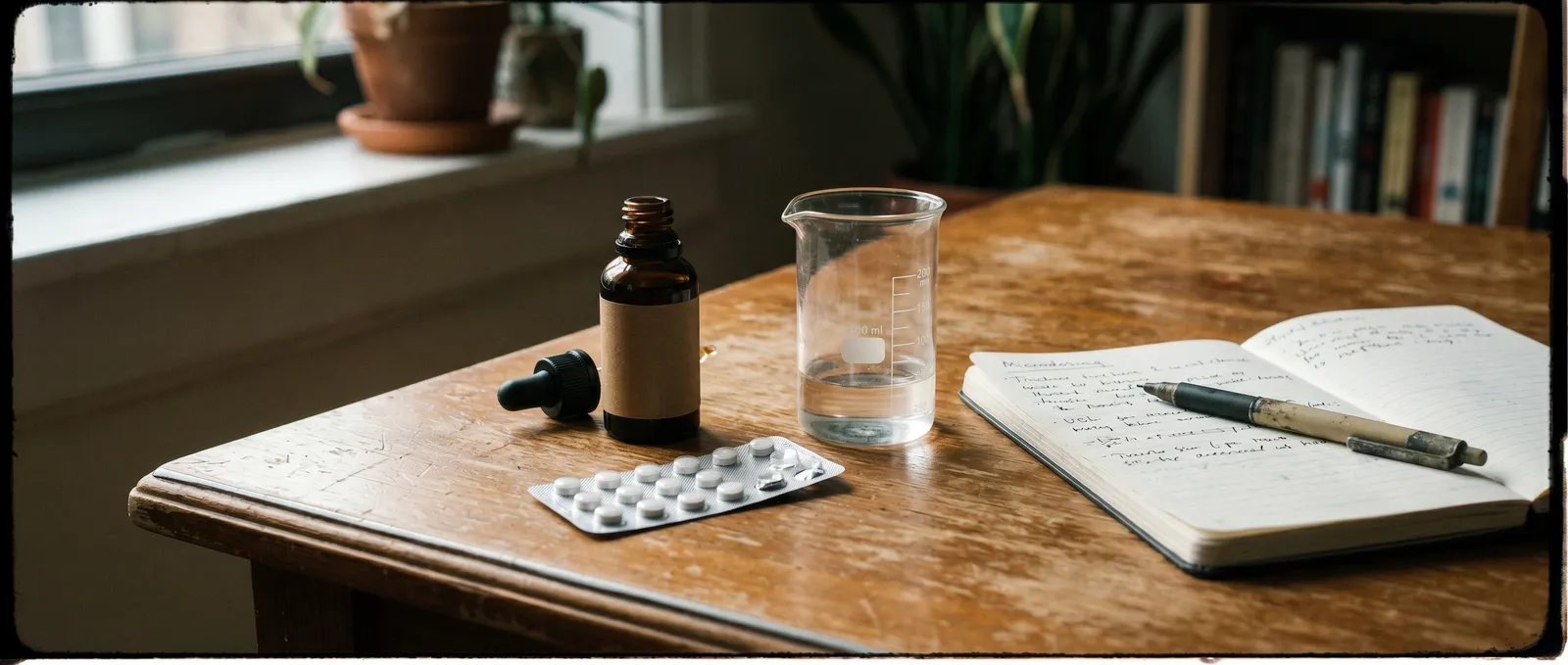
Food. An empty stomach absorbs psilocybin faster, which can push a borderline dose into perceptual territory. A light meal 30–60 minutes beforehand smooths the absorption curve. Nothing complicated — toast, a banana, yoghurt.
Journalling. This sounds soft, but it's one of the most practical tools available. Note the date, dose, time taken, sleep quality the night before, mood before dosing, and mood at the end of the day. After 4 weeks, you have actual data instead of vague impressions. You'll spot patterns — both positive and negative — that you'd otherwise miss entirely.
Caffeine and other stimulants. Psilocybin is a serotonin receptor agonist. Caffeine is an adenosine antagonist. They don't interact dangerously, but stacking stimulants on a microdose day can produce anxiety or jitteriness that gets misattributed to the microdose itself. If you drink coffee, keep your intake consistent across dose days and rest days so you can isolate variables.
Step 4: Screen for Contraindications Before You Start
Contraindication screening is the non-negotiable first step before any microdosing protocol begins. This step comes before step 1 in practice — but people skip it, so it gets its own section here.
Psilocybin and LSD both act primarily on serotonin receptors (5-HT2A). If you're taking any medication that also affects the serotonin system — SSRIs, SNRIs, MAOIs, lithium, tramadol — you have a potential interaction that ranges from "the microdose won't work" to "serotonin syndrome," which is a medical emergency. The dedicated article on microdosing drug interactions covers the specifics in full; the short version is: if you take psychiatric medication, do not start a microdosing harm reduction protocol without understanding the pharmacological overlap.
Personal and family history of psychotic disorders (schizophrenia, bipolar I with psychotic features) is a firm contraindication even at microdose levels. The research base here is thin — most studies exclude these populations — but the precautionary principle applies, and the risk-benefit ratio doesn't justify experimentation. The Beckley Foundation has consistently emphasised the importance of psychiatric screening in any psychedelic research context, and the same logic applies to self-directed microdosing.
Cardiac conditions deserve a mention too. Psilocybin binds to 5-HT2B receptors, which are expressed in heart valve tissue. At full psychoactive doses taken occasionally, this is not considered clinically significant. At microdose levels taken repeatedly over months, the long-term cardiac data simply doesn't exist yet. This is an area where the science hasn't caught up with the practice.
Step 5: Start Low and Calibrate
Starting at the lowest plausible dose and adjusting upward is the safest calibration method. Research protocols have used a range, not a single number, because individual sensitivity varies by body weight, metabolism, genetics (CYP2D6 enzyme activity affects psilocin clearance), and even gut microbiome composition. The microdosing harm reduction approach: start at the bottom of the range and adjust upward over two or three dose days.
For psilocybin truffles, that means beginning around 0.5 g of fresh material (roughly 0.05 g dried equivalent). If you feel nothing — not emotionally, not perceptually, nothing — on three consecutive dose days at that level, nudge up by 0.25 g. The ceiling for a microdose is the point just below perceptual threshold. If you overshoot, you haven't ruined anything — just note it, skip the next dose day, and drop back down.
For LSD, volumetric dosing (dissolving a known-quantity tab in distilled water or vodka and measuring with a graduated syringe) is the only reliable method. Cutting a tab into quarters introduces massive inconsistency because LSD is not evenly distributed across blotter paper.
Step 6: Monitor for Warning Signs
Recognising early warning signs is what prevents a benign protocol from becoming a problematic habit. Most microdosing experiences are uneventful by design — that's the point. But harm reduction means knowing when to stop.
Stop or pause if you notice:
- Increased anxiety that persists on rest days (not just dose days)
- Sleep disruption lasting more than a week
- Emotional blunting — feeling flat rather than subtly enhanced
- Increasing the dose more than twice in a cycle to "feel something"
- Difficulty distinguishing dose days from rest days (possible tolerance plateau)
- Any perceptual disturbance that doesn't resolve within 4–6 hours
The Rootman et al. (2021) survey found that the three most commonly reported challenges were physiological discomfort (experienced by ~18% of respondents), increased anxiety (~7%), and impaired focus (~9%). These numbers are relatively low, but they're not zero — and they rise when people skip rest days or escalate doses.
A microdosing protocol is not a commitment you have to see through. If it's not working, or if it's producing more friction than benefit, stopping is the correct microdosing harm reduction decision. There is no withdrawal syndrome associated with discontinuing psilocybin or LSD microdoses.
Step 7: Manage Set and Setting — Even at Sub-Perceptual Doses
Set and setting shape the microdosing experience even when the dose is sub-perceptual. "Set" at microdose levels means your baseline mental state and your intention for the protocol. Are you doing this out of curiosity? To support a creative practice? Because you read an article and thought "why not"?

None of those are wrong reasons, but vague intentions make it harder to evaluate whether the protocol is doing anything useful. "I want to see if my afternoon energy dips less on dose days" is a testable intention. "I want to feel better" is not.
"Setting" at microdose levels means your daily environment. A microdose on a calm work-from-home day and a microdose before a high-stress presentation are pharmacologically identical but experientially different. The substance amplifies what's already there — even at sub-perceptual levels, some users report that stressful contexts feel slightly more stressful on dose days. Schedule your first few dose days for low-stakes environments until you know your response.
What to Get for a Microdosing Setup
Before you order anything, make sure you have the essentials. A 0.01 g precision scale is non-negotiable — you can buy one for under €20. Microdosing truffles (such as the Microdosing XP pack available at Azarius) come in pre-portioned strips, which reduces variability but doesn't eliminate the need for a scale entirely. If you're following the Stamets Stack, you'll also want lion's mane capsules — Azarius carries several options. A small notebook or journalling app rounds out the kit.

What We Don't Know Yet
We'd be doing you a disservice if we pretended the science on microdosing harm reduction is settled. It isn't. Most published studies rely on self-report data from self-selected populations — people who already believe microdosing works. The Imperial College self-blinding study (Szigeti et al., 2022) was a landmark precisely because it showed how large the placebo component can be. Long-term safety data beyond 12 months doesn't exist in any controlled form. The 5-HT2B cardiac question remains genuinely open. And the interaction between microdosing and common supplements (omega-3s, adaptogens, nootropics) is almost entirely unstudied. This guide gives you the best available framework, but "best available" is not the same as "complete."
Common Mistakes
Eyeballing doses. "About this much" is not a measurement. A 0.01 g precision scale costs under €20 and eliminates the single biggest source of accidental overdosing.
Stacking supplements without research. The Stamets Stack (psilocybin + lion's mane + niacin) is popular, but the combination has not been studied in controlled trials. Adding other serotonergic supplements — 5-HTP, St. John's Wort, Syrian rue — on top of a microdose introduces unpredictable pharmacological interactions.
Treating microdosing as a substitute for professional support. If you're managing a diagnosed condition — depression, PTSD, ADHD — a microdosing protocol is not a treatment plan. The clinical trials showing psilocybin's therapeutic potential (e.g., Carhart-Harris et al., 2021, using 25 mg synthetic psilocybin for treatment-resistant depression) used full doses in supervised clinical settings with psychological support, not self-administered microdoses at home.
Never taking a break. Protocols have end dates for a reason. Running indefinitely without a washout period makes it impossible to distinguish pharmacological effects from habit, expectation, and lifestyle changes you may have made concurrently.
Last updated: April 2026
Frequently Asked Questions
10 questionsHow do I know if my microdose is too high?
Can I microdose every day?
Should I keep a microdosing journal?
Is it safe to microdose while taking antidepressants?
How long should a microdosing cycle last?
Do I need a precision scale for microdosing?
Can microdosing build tolerance over time?
Does potency vary between different truffle or mushroom batches?
Should I avoid driving or operating machinery on a microdose?
Can I microdose if I have a family history of psychosis or bipolar disorder?
About this article


Joshua Askew serves as Editorial Director for Azarius wiki content. He is Managing Director at Yuqo, a content agency specialising in cannabis, psychedelics and ethnobotanical editorial work across multiple languages. Th
This wiki article was drafted with AI assistance and reviewed by Joshua Askew, Managing Director at Yuqo. Editorial oversight by Adam Parsons.
Medical disclaimer. This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before use of any substance.
Last reviewed April 19, 2026
References (7)
- [1]Kuypers, K.P.C. et al. (2019). "Microdosing psychedelics: More questions than answers? An overview and suggestions for future research." Journal of Psychopharmacology, 33(9), 1039–1057.
- [2]Hutten, N.R.P.W. et al. (2019). "Dose-finding study for LSD microdosing." European Neuropsychopharmacology, 29, S653.
- [3]Szigeti, B. et al. (2022). "Self-blinding citizen science to explore psychedelic microdosing." eLife, 10, e62878.
- [4]Rootman, J.M. et al. (2021). "Adults who microdose psychedelics report health related motivations and lower levels of anxiety and depression compared to non-microdosers." Scientific Reports, 11, 22479.
- [5]Carhart-Harris, R.L. et al. (2021). "Trial of Psilocybin versus Escitalopram for Depression." New England Journal of Medicine, 384(15), 1402–1411.
- [6]European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). "New psychoactive substances and emerging trends." Accessed April 2026.
- [7]Beckley Foundation. "Psychedelic Research Programme: Safety and Screening Protocols." Accessed April 2026.
Related Articles
Microdosing Silicon Valley History: How Sub-Perceptual Doses Went from Fringe to Boardroom
Sub-perceptual psychedelic dosing and Silicon Valley share roots stretching back to the 1960s, when engineers at Menlo Park research labs first combined LSD…

Microdosing vs Macrodosing
Microdosing vs macrodosing is a comparison between two psychedelic dosing strategies that use the same substances at vastly different levels — microdosing…

Microdosing Myths and Misconceptions
Microdosing myths and misconceptions is a category of persistent misinformation that has grown alongside the practice itself.

Microdosing When Inadvisable
Microdosing when inadvisable is a harm-reduction framework that identifies the specific medical, psychiatric, pharmacological, and situational circumstances…

Microdosing Protocols Fadiman Stamets: Full Comparison Guide
A microdosing protocol is a structured schedule dictating dose days and rest days, designed to produce sub-perceptual cognitive shifts without tolerance buildup.
The Microdosing Placebo Debate: How to Tell If It's Actually Working
The microdosing placebo debate is a scientific and practical controversy that examines whether sub-perceptual doses of psilocybin or LSD produce genuine…
Origin of Microdosing Fadiman: How His Protocol Became the Standard
The origin of microdosing as a formalised practice traces to James Fadiman's 2011 book The Psychedelic Explorer's Guide, which introduced sub-perceptual…
Microdosing Research Current State
The current state of microdosing research reveals a field caught between enthusiastic self-reports and sobering controlled data.

Microdosing Medication Interactions
Microdosing medication interactions describe how sub-perceptual doses of psilocybin or LSD affect — or are affected by — prescribed drugs.