This article discusses psychoactive substances intended for adults (18+). If you have a health condition or take medication, consult a doctor before use. Our age policy
What Is Microdosing?
Definition
Microdosing means taking one-tenth to one-twentieth of a standard psychedelic dose — typically 0.1–0.3 g dried psilocybin mushroom or 5–20 micrograms of LSD — on a regular schedule. The aim is sub-perceptual: subtle shifts in mood and focus without altered perception. A self-blinding study by Szigeti et al. (2021) found improvements were statistically indistinguishable from placebo, making this one of the most debated practices in modern psychedelic science.
18+ only
Microdosing is the practice of regularly taking sub-perceptual amounts of a psychedelic substance — typically one-tenth to one-twentieth of a full dose — on a fixed schedule over several weeks. The goal is not to alter perception but to produce subtle shifts in mood, focus, or creative thinking. According to a systematic review by Kuypers et al. (2019), reported benefits include improved well-being and cognition, though controlled trials remain scarce and placebo effects are significant. This guide is written for adults aged 18 and over; the dosing ranges described below apply to adult physiology.
Key Facts
- Substances most commonly microdosed: psilocybin (from mushrooms or truffles) and LSD (lysergic acid diethylamide), with emerging interest in mescaline, DMT, and THC (Hutten et al., 2019).
- Typical psilocybin microdose: approximately 0.1–0.3 g dried mushroom or equivalent truffle weight — roughly 1–3 mg psilocybin (Fadiman & Korb, 2019).
- Typical LSD microdose: 5–20 micrograms, compared to a full dose of 100–200 micrograms (Yanakieva et al., 2019).
- Primary receptor activity: psilocin (the active metabolite of psilocybin) and LSD both act as partial agonists at serotonin 5-HT2A receptors (Nichols, 2016).
- Prevalence: a Global Drug Survey (2019) analysis found that 1 in 4 psychedelic users had microdosed in the past 12 months.
- Placebo problem: the largest placebo-controlled self-blinding study (Szigeti et al., 2021) found that improvements in well-being were statistically indistinguishable between microdose and placebo groups.
- Side effects: reported adverse effects include mild increases in blood pressure, transient anxiety, and difficulty sleeping, most of which resolve within hours (Anderson et al., 2019).
Commercial Disclosure
Azarius sells psilocybin truffle products and has a commercial interest in this topic. Our editorial process includes independent pharmacological review to mitigate commercial bias.
Who Should Not Microdose
Certain populations face elevated risk. According to Johnson et al. (2018), screening criteria for psilocybin research typically exclude the following groups — and those exclusions apply equally to unsupervised microdosing:

- Personal or family history of psychotic disorders (schizophrenia, bipolar I). Serotonin 5-HT2A agonism can trigger or worsen psychotic episodes (Rucker et al., 2018).
- Pregnancy and breastfeeding. No safety data exists for sub-perceptual psychedelic doses during pregnancy.
- Current SSRI or SNRI use. Combining serotonergic psychedelics with SSRIs may blunt effects or, in rare cases, contribute to serotonin syndrome (Malcolm & Thomas, 2022).
- Lithium use. Case reports link lithium + psychedelics to seizures (Nayak et al., 2021).
- MAOI use. MAOIs potentiate tryptamine psychedelics unpredictably — a standard microdose could become a full dose.
- Cardiovascular conditions. Both psilocybin and LSD produce mild, transient increases in heart rate and blood pressure (Holze et al., 2022).
- Under 18. No clinical microdosing data exists for adolescents, and the developing brain's serotonergic system responds differently to 5-HT2A agonists.
History and Origin
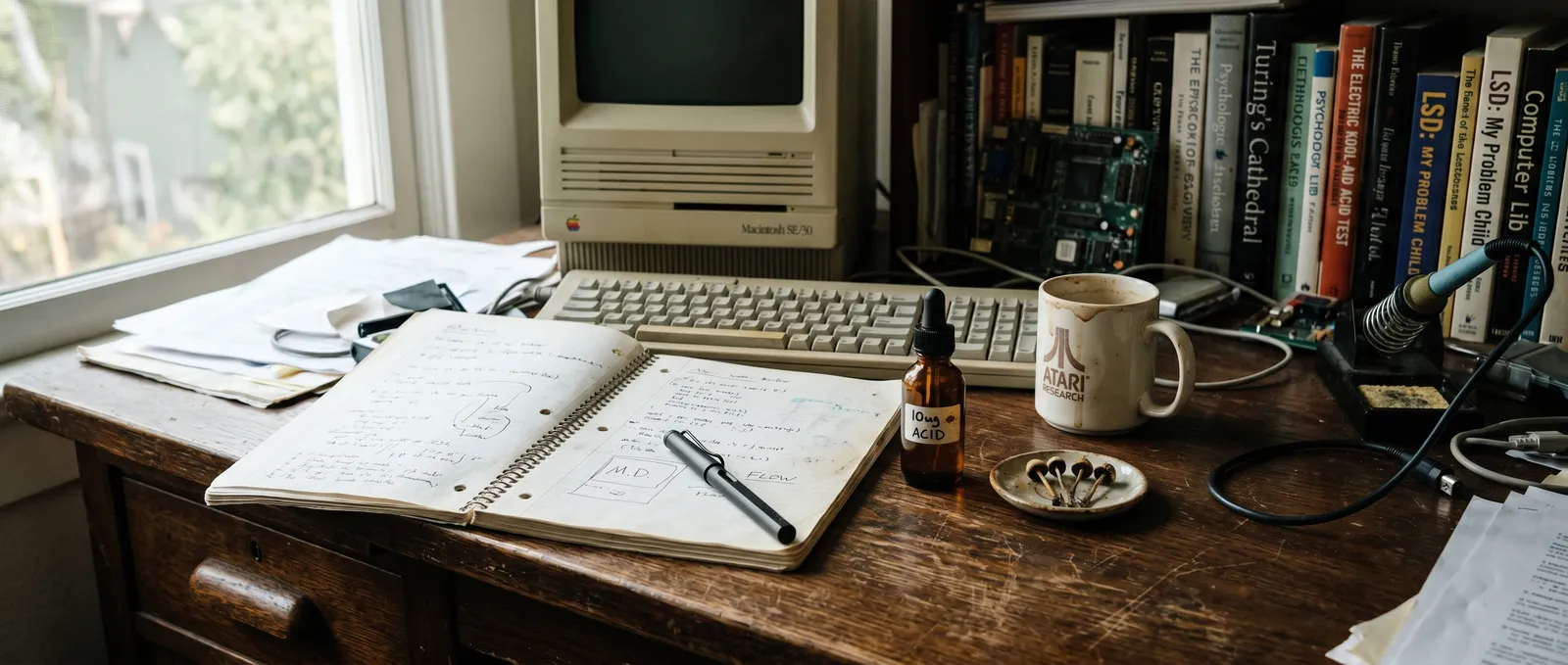
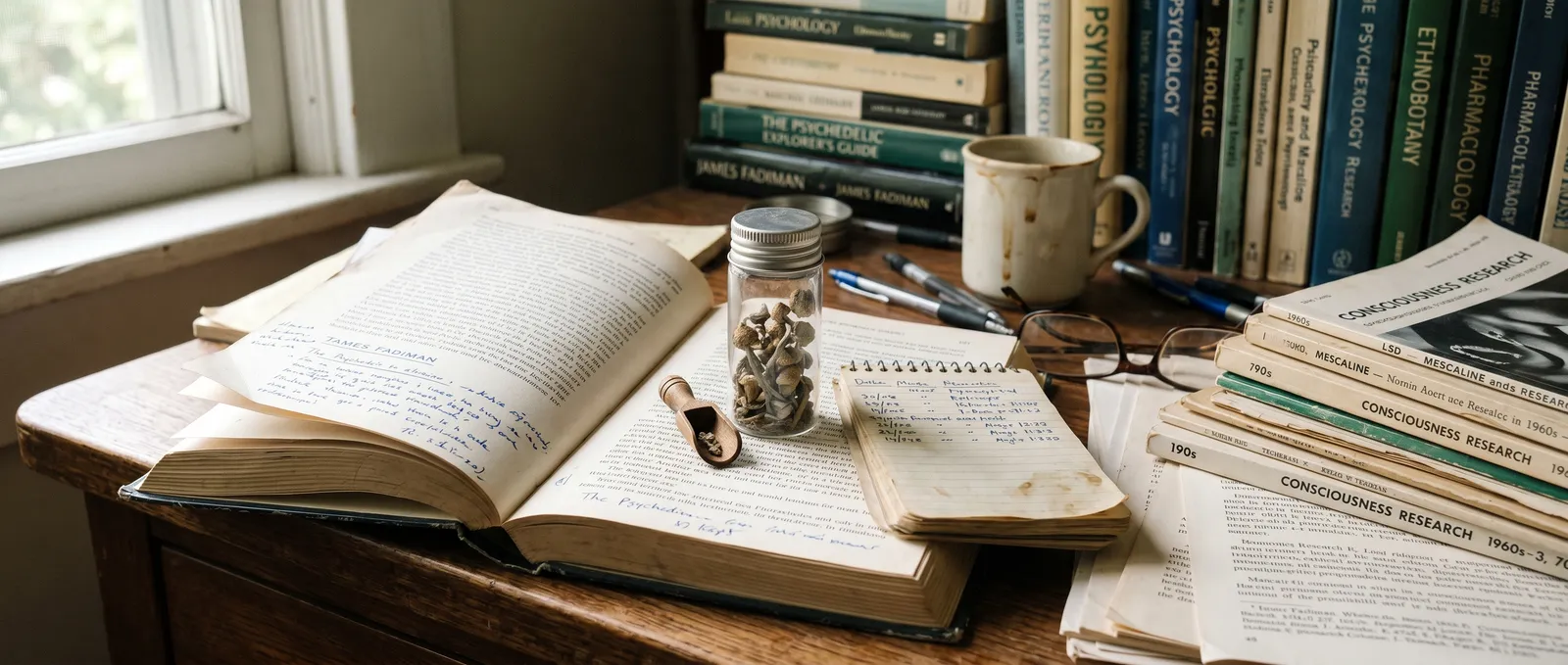
The word "microdosing" entered popular vocabulary around 2011, but the practice is older than the term. Albert Hofmann, the Swiss chemist who synthesised LSD in 1938, reportedly took very low doses of LSD during the final decades of his life, describing them as sharpening his thinking on afternoon walks (Fadiman, 2011). The modern microdosing movement traces largely to James Fadiman's 2011 book The Psychedelic Explorer's Guide, which proposed a specific protocol — one dose day followed by two rest days — and began collecting self-reports from hundreds of volunteers.

By 2015, microdosing had spread from Silicon Valley biohacker circles into mainstream media. Ayelet Waldman's 2017 memoir A Really Good Day brought the concept to a non-technical audience. The first controlled laboratory study of LSD microdosing (Yanakieva et al., 2019) appeared years after the practice was already widespread — a pattern where popular use outpaced scientific evidence.
How Microdosing Works — Active Compounds and Receptor Activity
The two most commonly microdosed substances share a core mechanism: partial agonism at serotonin 5-HT2A receptors in the prefrontal cortex. At full doses, this produces the perceptual distortions and ego dissolution associated with a psychedelic experience. At microdose levels, the receptor activation is far lower — the hypothesis is that it modulates neural plasticity and connectivity without crossing the perceptual threshold.

| Compound | Source | Primary receptor | Ki at 5-HT2A | Onset (oral) | Duration |
|---|---|---|---|---|---|
| Psilocin (from psilocybin) | Psilocybe mushrooms, sclerotia (truffles) | 5-HT2A partial agonist | ~6 nM (Rickli et al., 2016) | 30–60 min | 4–6 hours |
| LSD | Synthetic (ergot alkaloid derivative) | 5-HT2A partial agonist | ~3.5 nM (Rickli et al., 2016) | 30–90 min | 8–12 hours |
| Mescaline | San Pedro, Peyote cacti | 5-HT2A partial agonist | ~4,900 nM | 45–120 min | 8–12 hours |
Psilocybin itself is a prodrug — your liver converts it to psilocin via dephosphorylation. This is why onset varies with stomach contents and individual metabolism. LSD, by contrast, is active as-is and has an unusually long receptor residence time: the molecule gets physically trapped in the 5-HT2A binding pocket by a "lid" formed by extracellular loop 2, which partly explains its 8–12 hour duration even at microdose levels (Wacker et al., 2017). Much of the proposed neuroplasticity mechanism at sub-perceptual doses remains theoretical — the receptor binding data comes from full-dose pharmacology, and whether the same downstream signalling cascades activate at one-tenth the dose is not yet confirmed in human studies.
What to Expect — Effects at Microdose Levels
A properly calibrated microdose should be sub-perceptual — meaning you should not feel "altered" in any obvious way. The reported effects are subtle and often only noticed in retrospect. According to a large observational study by Anderson et al. (2019) involving 278 microdosers:
- Most commonly reported benefits: improved mood (26.6%), improved focus (14.8%), improved creativity (12.9%).
- Most commonly reported challenges: physiological discomfort such as headache or nausea (18.0%), increased anxiety (6.7%), worse mood on off-days (2.8%).
| Substance | Onset | Peak effects | Total duration | Common subjective reports |
|---|---|---|---|---|
| Psilocybin (truffle/mushroom) | 30–60 min | 1–2 hours | 4–5 hours | Slight mood lift, mild visual "brightness," easier flow state |
| LSD | 30–90 min | 2–4 hours | 8–10 hours | Increased energy, enhanced pattern recognition, mild stimulation |
| THC (cannabis) | 5–30 min (inhaled) / 45–90 min (oral) | 1–2 hours | 2–4 hours | Mild relaxation, slight appetite increase |
If you notice visual changes, body load, or difficulty concentrating, the dose is too high — that is a low recreational dose, not a microdose. The line between the two is thinner than most guides suggest, and individual sensitivity varies substantially.
Dosage Guide — Observed Ranges in Published Literature
All figures below are drawn from clinical studies and published survey data. Individual responses vary with body weight, metabolism, substance potency, and prior exposure. Psilocybin content in mushrooms and truffles is not uniform — even within the same batch.
| Level | Psilocybin (dried mushroom equivalent) | Psilocybin (fresh truffle equivalent) | LSD | THC (oral) |
|---|---|---|---|---|
| Threshold | 0.05–0.1 g | 0.3–0.7 g | 5 mcg | 1 mg |
| Light microdose | 0.1–0.15 g | 0.7–1.0 g | 5–10 mcg | 1–2.5 mg |
| Standard microdose | 0.15–0.3 g | 1.0–2.0 g | 10–20 mcg | 2.5–5 mg |
| Upper microdose | 0.3–0.5 g | 2.0–3.0 g | 20–25 mcg | 5–7.5 mg |
| Museum dose (low recreational) | 0.5–1.0 g | 3.0–5.0 g | 25–50 mcg | 7.5–15 mg |
The standard psilocybin microdose in published literature clusters around 0.1–0.3 g dried mushroom, which translates to roughly 1–3 mg of psilocybin (Fadiman & Korb, 2019). For fresh truffles (sclerotia), psilocybin content is lower per gram than dried mushrooms due to water content — typically 0.5–1.0% psilocybin by dry weight in truffles versus 0.5–2.0% in Psilocybe cubensis mushrooms (Gotvaldova et al., 2022). This is why truffle microdose weights are higher than dried mushroom weights for comparable effects.
Step-by-Step: Common Microdosing Protocols
Three structured schedules dominate the published literature and self-report databases. None has been validated in a large randomised controlled trial — they originate from practitioner recommendation and community consensus.
Step 1 — Choose a protocol
The Fadiman Protocol (Fadiman, 2011): Dose on Day 1, rest on Days 2–3, dose again on Day 4. Repeat for 4–8 weeks, then take a 2–4 week break. This is the most widely studied schedule in observational research.
The Stamets Stack (Stamets, 2018): Dose psilocybin alongside lion's mane mushroom and niacin (vitamin B3) for 4 consecutive days, then rest for 3 days. Paul Stamets hypothesises that niacin's vasodilatory effect pushes psilocin to peripheral nerve endings — this remains unproven in any controlled trial.
Every-other-day protocol: Dose on Day 1, rest on Day 2, repeat. Reported in Hutten et al. (2019) survey data. Some users prefer this for consistency.
Step 2 — Calibrate your dose
Start at the threshold range on a day with no obligations. If you feel perceptual changes — walls breathing, colours intensifying, thought loops — the dose is too high. Reduce by 25–50% next time. The target is sub-perceptual: you should be uncertain whether you took anything at all.
Step 3 — Standardise your material
Psilocybin content varies between mushroom species, between individual mushrooms, and even between the cap and stem of the same specimen. Grinding dried material into a fine powder and mixing thoroughly ("homogenising") reduces batch variation. Published analytical data shows psilocybin content can vary 2–4x within a single flush (Gotvaldova et al., 2022). Truffles tend to be more consistent than mushrooms because they grow as a single dense mass rather than individual fruiting bodies, but variation still exists.
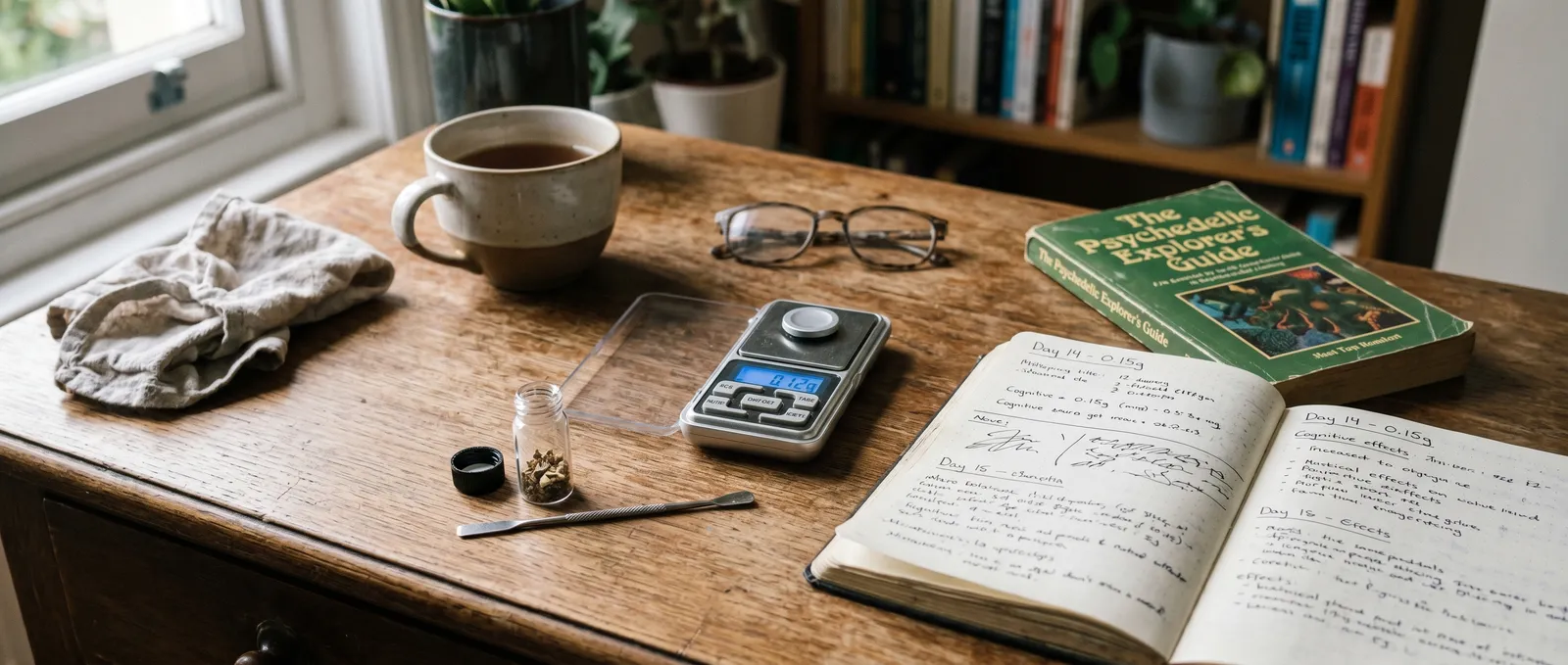
Step 4 — Track your experience
Keep a simple daily log: mood (1–10), energy (1–10), sleep quality, any side effects. The Fadiman research protocol asks participants to journal for the full cycle. This is also how you separate genuine effects from expectation — if you are logging honestly, patterns (or the absence of them) become visible after 3–4 weeks.
Step 5 — Take breaks
All published protocols include rest periods. Serotonin 5-HT2A receptors downregulate with repeated agonist exposure — tolerance builds within days at full doses. Whether meaningful tolerance develops at microdose levels is unclear, but scheduled breaks are standard practice across all protocols.
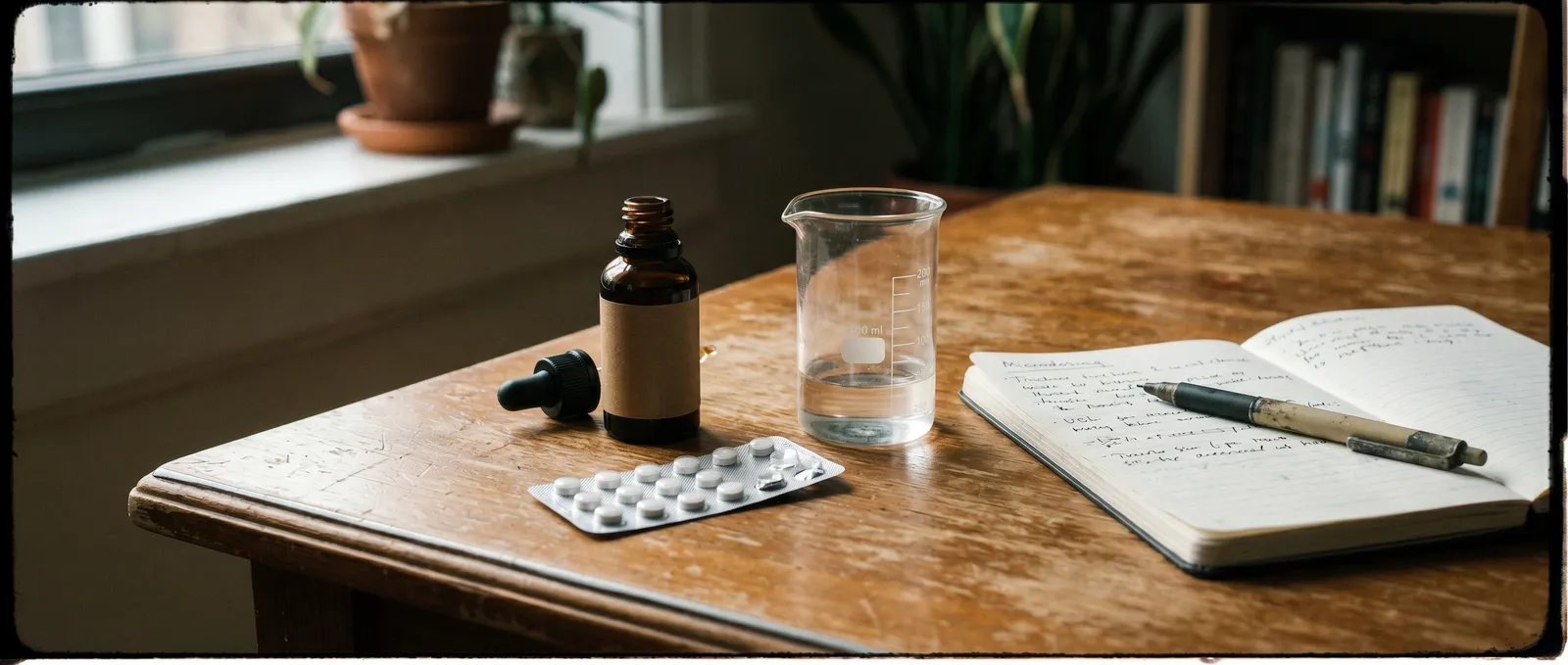
Preparation Methods
Dried mushroom powder in capsules: The most common method in self-report studies. Grind dried material, homogenise, weigh individual doses on a milligram scale (0.001 g precision), and fill into empty gelatin or vegetable capsules. This eliminates taste and improves dose consistency.
Fresh truffle: Weigh on a precision scale. Fresh truffles contain approximately 50–70% water, so 1 g fresh truffle is roughly equivalent to 0.3–0.5 g dried. Some people eat them directly; others steep them in warm (not boiling) water for 10–15 minutes as a tea, which may speed onset slightly.
Volumetric dosing for LSD: Because LSD doses are measured in micrograms and blotter paper is not uniformly dosed, some microdosers dissolve a known-quantity tab in distilled water or vodka (e.g., one 100 mcg tab in 10 ml), then measure out 1 ml (10 mcg) with a graduated syringe. This approach is described in Fadiman & Korb (2019) and improves dose precision substantially.
THC edibles: Commercial low-dose edibles (1–2.5 mg THC per unit) exist in some markets. For homemade preparations, achieving consistent 1–2 mg doses is extremely difficult without laboratory testing.
Safety, Side Effects, and Drug Interactions
The physiological safety profile of classical psychedelics at microdose levels appears favourable in published data — but "appears" is doing heavy lifting in that sentence. Most safety data comes from self-selected survey respondents, not controlled trials. The largest prospective study to date (Szigeti et al., 2021, n=191) found no serious adverse events, but participants were self-screened and generally healthy.
Reported side effects
Anderson et al. (2019) catalogued the following in 278 microdosers over 6 weeks:
- Physiological discomfort (headache, nausea, temperature sensitivity): 18.0%
- Increased anxiety: 6.7%
- Impaired focus (opposite of intended effect): 4.2%
- Impaired energy or mood on off-days: 2.8%
- Mild increases in blood pressure and heart rate: reported in controlled LSD microdose studies (Holze et al., 2022)
Most adverse effects were mild and transient, resolving within hours of dosing. No hospitalisations or psychiatric emergencies were reported in any published microdosing study as of early 2025, though reporting bias is likely — people who have bad reactions may drop out of studies or stop responding to surveys.
Drug interactions
Fadiman and Korb compiled interaction data from their ongoing self-report database. The table below synthesises their findings with published pharmacological data:
| Medication / substance | Interaction type | Risk level | Notes |
|---|---|---|---|
| Lithium | Seizure risk, unpredictable potentiation | Severe | Case reports of seizures with LSD + lithium (Nayak et al., 2021). Avoid entirely. |
| MAOIs (phenelzine, tranylcypromine, moclobemide) | Potentiation of tryptamine psychedelics | Severe | MAOIs inhibit psilocin metabolism — a microdose could become a full dose. Also applies to ayahuasca-containing brews. |
| Tramadol | Serotonin syndrome risk, seizure threshold lowering | High | Tramadol is serotonergic; combining with 5-HT2A agonists increases serotonin syndrome risk. |
| SSRIs (fluoxetine, sertraline, etc.) | Blunted psychedelic effects; theoretical serotonin syndrome risk | Moderate | Most Fadiman protocol respondents on SSRIs reported reduced or absent effects (Malcolm & Thomas, 2022). Do not discontinue SSRIs to microdose — SSRI withdrawal carries its own serious risks. |
| SNRIs (venlafaxine, duloxetine) | Similar to SSRIs — blunting plus serotonergic interaction | Moderate | Less data than SSRIs. Same caution applies. |
| Cannabis | Potentiation of anxiety and perceptual effects | Moderate | THC can amplify psychedelic effects unpredictably, even at microdose levels. |
| Caffeine | Mild increase in stimulation and anxiety | Low | Most microdosers continue normal caffeine intake without issues. Some report heightened jitteriness. |
| CBD | Possible anxiolytic modulation | Low | No published interaction data specific to microdosing. CBD does not act on 5-HT2A. |
This table is not exhaustive. Psychedelic pharmacology at sub-threshold doses is poorly characterised, and most interaction data is extrapolated from full-dose studies or anecdotal reports. If you take any regular medication, discuss the specific combination with a pharmacist or physician who is familiar with the substances involved.
The Placebo Question — Can We Trust the Research?
This is the most honest section in any microdosing guide, and the one most often skipped. The short answer: we do not yet know whether microdosing works beyond placebo.
The landmark self-blinding study by Szigeti et al. (2021), published in eLife, asked 191 participants to create their own placebo-controlled setup using opaque capsules. Both the microdose group and the placebo group reported statistically significant improvements in well-being, cognitive function, and emotional stability. The difference between the two groups was not significant. This does not prove microdosing "doesn't work" — it proves that expectation is a powerful variable that existing studies have not adequately controlled for.
A controlled laboratory study by Marschall et al. (2022) found that repeated low doses of psilocybin (0.5 mg — roughly equivalent to 0.15 g dried mushroom) did not produce significant changes in creativity, well-being, or cognition compared to placebo over a two-week period. Meanwhile, a separate controlled study by Hutten et al. (2020) found that low-dose LSD (5–20 mcg) produced dose-dependent changes in time perception and subjective drug effects — confirming that microdoses are pharmacologically active, even if the downstream benefits remain unproven.
The gap between "pharmacologically active" and "therapeutically useful" is where the honest uncertainty sits. Microdoses do something — the receptor binding data and subjective drug effect measures confirm that. Whether that something translates into the mood, creativity, and focus improvements that thousands of self-reporters describe, or whether those improvements are driven by expectation, ritual, and the act of paying attention to your own mental state — that question remains genuinely open.
Emergency Information
If you or someone you know experiences a severe reaction — persistent panic, chest pain, confusion, or signs of serotonin syndrome (agitation, rapid heart rate, muscle rigidity, high temperature) — contact emergency services immediately.
- Netherlands: 112 (general emergency) or the Dutch Poisons Information Centre: 030-274 8888
- Germany: 112 or Giftnotruf Berlin: 030-19240
- Belgium: 112 or Antigifcentrum: 070-245 245
- France: 15 (SAMU) or 112
- UK: 999 or 111 (NHS non-emergency)
- International: your local emergency number
Tell medical staff exactly what was taken, how much, and when. They are there to help, not to judge. Bring the substance or packaging if possible.
Last updated: April 2026
Frequently Asked Questions
9 questionsWhat happens when you take a microdose?
What is the difference between microdosing and macrodosing?
Can you microdose while taking antidepressants?
How long should a microdosing cycle last?
Is there scientific evidence that microdosing actually works?
What substances are most commonly used for microdosing?
Who should not try microdosing?
Can you build a tolerance to microdosing?
Does microdosing show up on a drug test?
About this article


Joshua Askew serves as Editorial Director for Azarius wiki content. He is Managing Director at Yuqo, a content agency specialising in cannabis, psychedelics and ethnobotanical editorial work across multiple languages. Th
This wiki article was drafted with AI assistance and reviewed by Joshua Askew, Managing Director at Yuqo. Editorial oversight by Adam Parsons.
Medical disclaimer. This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before use of any substance.
Last reviewed April 19, 2026
References (16)
- [1]Anderson, T., Petranker, R., Christopher, A., et al. (2019). Psychedelic microdosing benefits and challenges: an empirical codebook. Harm Reduction Journal, 16(1), 43.
- [2]Fadiman, J. (2011). The Psychedelic Explorer's Guide: Safe, Therapeutic, and Sacred Journeys. Park Street Press.
- [3]Fadiman, J. & Korb, S. (2019). Might microdosing psychedelics be safe and beneficial? An initial exploration. Journal of Psychoactive Drugs, 51(2), 118–122.
- [4]Gotvaldova, K., Hajkova, K., Borovicka, J., & Jurok, R. (2022). Stability of psilocybin and its four analogs in the biomass of the psychotropic mushroom Psilocybe cubensis. Drug Testing and Analysis, 14(2), 302–310.
- [5]Holze, F., Ley, L., Muller, F., et al. (2022). Direct comparison of the acute effects of lysergic acid diethylamide and psilocybin in a double-blind placebo-controlled study in healthy subjects. Neuropsychopharmacology, 47(6), 1180–1187.
- [6]Hutten, N.R.P.W., Mason, N.L., Dolder, P.C., & Kuypers, K.P.C. (2019). Motives and side-effects of microdosing with psychedelics among users. International Journal of Neuropsychopharmacology, 22(7), 426–434.
- [7]Johnson, M.W., Richards, W.A., & Griffiths, R.R. (2018). Human hallucinogen research: guidelines for safety. Journal of Psychopharmacology, 22(6), 603–620.
- [8]Kuypers, K.P.C., Ng, L., Erritzoe, D., et al. (2019). Microdosing psychedelics: more questions than answers? An overview and suggestions for future research. Journal of Psychopharmacology, 33(9), 1039–1057.
- [9]Malcolm, B. & Thomas, K. (2022). Serotonin toxicity of serotonergic psychedelics. Psychopharmacology, 239, 1881–1891.
- [10]Marschall, J., Fejer, G., Lempe, P., et al. (2022). Psilocybin microdosing does not affect emotion-related symptoms and processing: a preregistered field and lab-based study. Journal of Psychopharmacology, 36(1), 97–113.
- [11]Nayak, S.M., Gukasyan, N., Barrett, F.S., et al. (2021). Classic psychedelic coadministration with lithium, but not lamotrigine, is associated with seizures: an analysis of online psychedelic experience reports. Psychopharmacology, 238, 3281–3299.
- [12]Nichols, D.E. (2016). Psychedelics. Pharmacological Reviews, 68(2), 264–355.
- [13]Rickli, A., Moning, O.D., Hoener, M.C., & Liechti, M.E. (2016). Receptor interaction profiles of novel psychoactive tryptamines compared with classic hallucinogens. European Neuropsychopharmacology, 26(8), 1327–1337.
- [14]Szigeti, B., Kartner, L., Blemings, A., et al. (2021). Self-blinding citizen science to explore psychedelic microdosing. eLife, 10, e62878.
- [15]Wacker, D., Wang, S., McCorvy, J.D., et al. (2017). Crystal structure of an LSD-bound human serotonin receptor. Cell, 168(3), 377–389.
- [16]Yanakieva, S., Polychroni, N., Family, N., et al. (2019). The effects of microdose LSD on time perception: a randomised, double-blind, placebo-controlled trial. Psychopharmacology, 236, 1159–1170.
Related Articles
Microdosing Silicon Valley History: How Sub-Perceptual Doses Went from Fringe to Boardroom
Sub-perceptual psychedelic dosing and Silicon Valley share roots stretching back to the 1960s, when engineers at Menlo Park research labs first combined LSD…

Microdosing vs Macrodosing
Microdosing vs macrodosing is a comparison between two psychedelic dosing strategies that use the same substances at vastly different levels — microdosing…

Microdosing Myths and Misconceptions
Microdosing myths and misconceptions is a category of persistent misinformation that has grown alongside the practice itself.

Microdosing When Inadvisable
Microdosing when inadvisable is a harm-reduction framework that identifies the specific medical, psychiatric, pharmacological, and situational circumstances…

Microdosing Protocols Fadiman Stamets: Full Comparison Guide
A microdosing protocol is a structured schedule dictating dose days and rest days, designed to produce sub-perceptual cognitive shifts without tolerance buildup.
The Microdosing Placebo Debate: How to Tell If It's Actually Working
The microdosing placebo debate is a scientific and practical controversy that examines whether sub-perceptual doses of psilocybin or LSD produce genuine…
Origin of Microdosing Fadiman: How His Protocol Became the Standard
The origin of microdosing as a formalised practice traces to James Fadiman's 2011 book The Psychedelic Explorer's Guide, which introduced sub-perceptual…
Microdosing Research Current State
The current state of microdosing research reveals a field caught between enthusiastic self-reports and sobering controlled data.

Microdosing Medication Interactions
Microdosing medication interactions describe how sub-perceptual doses of psilocybin or LSD affect — or are affected by — prescribed drugs.