This article discusses psychoactive substances intended for adults (18+). If you have a health condition or take medication, consult a doctor before use. Our age policy
Ginkgo Biloba Cognitive Research Overview

Definition
Ginkgo biloba L. is the most widely studied botanical for cognitive function, with clinical trials spanning dementia prevention, existing impairment, and healthy-adult nootropic use. The two largest independent trials — GEM and GuidAge — found no benefit for dementia prevention (DeKosky et al., 2008; Vellas et al., 2012), while smaller meta-analyses suggest a modest effect in people with existing cognitive decline.
What the Research Actually Covers
Ginkgo biloba cognitive research is a body of clinical and preclinical investigation that examines whether standardised extracts of the world's oldest surviving tree species can meaningfully improve human memory, attention, and processing speed. Ginkgo biloba L. — the last surviving member of the Ginkgoaceae family, a lineage stretching back roughly 270 million years — is probably the single most studied botanical in the cognitive-performance space. Walk into any European pharmacy and you will find standardised ginkgo extract on the shelf. The question is whether the ginkgo biloba cognitive research behind it holds up under scrutiny, and the honest answer is: it depends entirely on who is taking it and what outcome you are measuring.

Most clinical work uses a standardised extract called EGb 761, produced by a single German manufacturer and containing approximately 24% flavone glycosides and 6% terpene lactones (ginkgolides A, B, C and bilobalide). When a study says "ginkgo," it almost always means this specific extract at 120–240 mg per day. That matters, because crude leaf preparations and EGb 761 are not pharmacologically interchangeable — the standardisation process removes ginkgolic acids (which are cytotoxic above certain thresholds) and concentrates the compounds thought to be active (DeKosky et al., 2008).
The research splits into three broad buckets: large-scale dementia-prevention trials in older adults, medium-term studies in people already showing cognitive decline, and shorter-term studies in healthy younger adults looking for a nootropic edge. The results across those three categories diverge sharply.
Large-Scale Prevention Trials: The GEM and GuidAge Studies
The two landmark prevention trials both returned negative results for dementia prevention, finding no significant benefit from standardised ginkgo extract over placebo (DeKosky et al., 2008; Vellas et al., 2012). The Ginkgo Evaluation of Memory study (GEM) in the United States and the GuidAge trial in France were both randomised, double-blind, placebo-controlled, and both enrolled thousands of participants over multiple years.
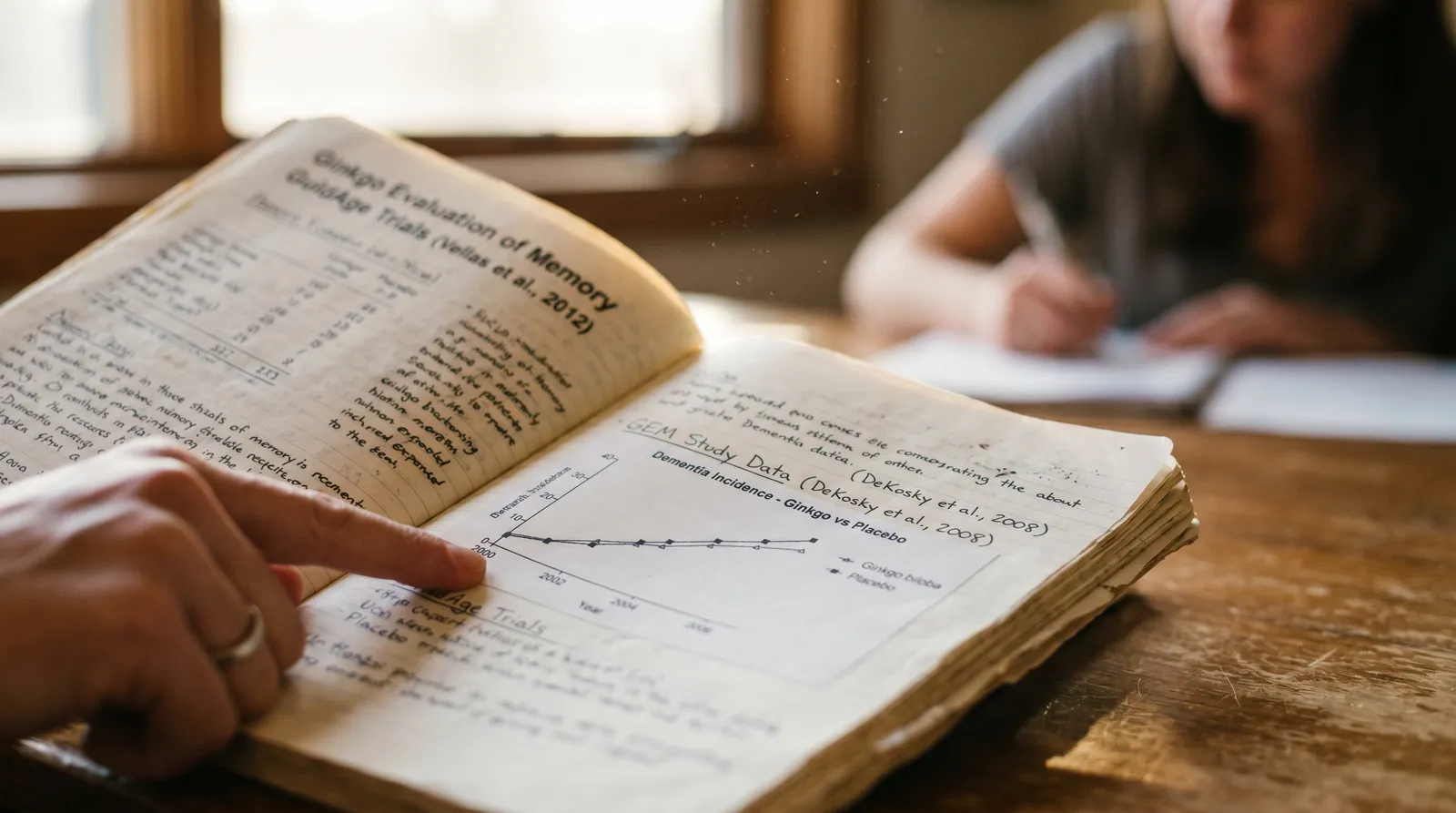
GEM enrolled 3,069 adults aged 72–96 with normal cognition or mild cognitive impairment and randomised them to 240 mg per day of EGb 761 or placebo. After a median follow-up of 6.1 years, ginkgo did not reduce the overall incidence rate of dementia or Alzheimer's disease compared to placebo (DeKosky et al., 2008). The hazard ratio was 1.12 (95% CI 0.94–1.33) — essentially no difference, and if anything a slight numerical trend in the wrong direction.
GuidAge, published four years later, followed 2,854 French adults aged 70 and over who had reported memory complaints to their GP. After five years of 240 mg EGb 761 daily, the incidence of Alzheimer's disease was not significantly different between groups (Vellas et al., 2012). A post-hoc subgroup analysis hinted at a possible reduction in Alzheimer's incidence among participants who adhered to treatment for at least four years, but post-hoc findings in a trial that missed its primary endpoint are hypothesis-generating at best — not evidence you would stake a recommendation on.
These two trials, between them enrolling nearly 6,000 older adults with years of follow-up, represent the strongest available ginkgo biloba cognitive research for dementia prevention. The conclusion is fairly clear: EGb 761 at standard doses does not appear to prevent the onset of dementia or Alzheimer's disease in older populations.
Existing Cognitive Impairment and Diagnosed Dementia
Ginkgo extract shows its most credible positive signal in people who already have measurable cognitive decline, with meta-analyses reporting modest but statistically significant improvements on standard cognitive scales (Birks & Grimley Evans, 2009; Tan et al., 2015). Here the evidence is more mixed, and some of it is genuinely positive — though the clinical meaningfulness is debated.

A Cochrane systematic review by Birks and Grimley Evans (2009) assessed 36 trials of ginkgo for cognitive impairment and dementia. The overall conclusion was cautious: there was "inconsistent and unconvincing" evidence of benefit, partly because the trials varied enormously in quality, dose, duration, and outcome measures. Some individual trials showed statistically significant improvements on cognitive subscales (particularly the SKT and ADAS-Cog), but the pooled effect was not robust enough for the reviewers to endorse clinical use.
More recent meta-analyses have been somewhat kinder. Tan et al. (2015) pooled data from nine randomised controlled trials totalling 2,561 patients with Alzheimer's disease or mild cognitive impairment and found that EGb 761 at 240 mg per day for at least 22 weeks produced a statistically significant improvement on the ADAS-Cog scale (weighted mean difference −2.86 points, 95% CI −3.18 to −2.54). For context, the ADAS-Cog runs from 0 to 70, and a 2–3 point change is generally considered the minimum clinically detectable difference — so the effect sits right at the threshold of what a patient or carer might actually notice.
A large systematic review of systematic reviews by Zhang et al. (2016) examined 18 meta-analyses of ginkgo biloba extracts and concluded that the evidence was "potentially positive" for cognitive function in patients with dementia, though the authors flagged heterogeneity across studies and potential publication bias as significant caveats. The positive signals came almost exclusively from trials using EGb 761 at 240 mg per day for 22 weeks or longer — shorter durations and lower doses showed little.
Healthy Younger Adults: The Nootropic Question
Healthy younger adults show no reliable cognitive benefit from ginkgo supplementation in well-designed trials (Laws et al., 2012). This is where the evidence gets thinnest and the marketing gets loudest. Plenty of ginkgo products are sold to university students and working professionals on the implicit promise of sharper memory and faster processing speed. The clinical data do not strongly support that promise.

Laws et al. (2012) conducted a meta-analysis specifically looking at ginkgo's effects on cognitive function in healthy individuals across all age groups. Across the included trials, ginkgo did not produce a statistically significant improvement on any standard measure of memory, attention, or executive function. The authors noted that some individual studies reported positive findings on specific subtests, but these did not survive pooling and were likely influenced by small sample sizes and selective reporting.
A handful of acute-dosing studies have shown modest short-term effects on attention and working memory within hours of a single dose. Kennedy et al. (2000) found that 360 mg of ginkgo extract improved speed of attention in healthy young volunteers, but the effect was not consistent across all cognitive domains tested and has not been reliably replicated. Single-dose studies are interesting for understanding pharmacokinetics but tell you very little about what happens with daily use over weeks or months.
The bottom line for healthy adults: if there is a cognitive benefit, it is small enough that well-designed trials have not been able to reliably detect it. That does not mean zero effect — absence of evidence is not evidence of absence — but it does mean the confidence interval includes zero, and anyone expecting a noticeable boost is likely to be disappointed.
How Ginkgo Is Thought to Work
The proposed mechanisms centre on platelet-activating factor antagonism, antioxidant neuroprotection, and cerebral blood-flow modulation, though none have been conclusively linked to clinical cognitive outcomes in humans (Braquet, 1987; Bastianetto et al., 2000). The two main compound classes — flavone glycosides (quercetin, kaempferol, and isorhamnetin derivatives) and terpene lactones (ginkgolides and bilobalide) — act through different pathways.

Ginkgolides, particularly ginkgolide B, are potent antagonists of platelet-activating factor (PAF), which gives ginkgo its antiplatelet activity (Braquet, 1987). PAF antagonism also has downstream effects on microcirculation, and improved cerebral blood flow is one of the oldest proposed mechanisms for ginkgo's cognitive effects. Neuroimaging studies have shown modest increases in regional cerebral blood flow following ginkgo administration, though whether this translates to functional cognitive improvement is the unresolved question (Santos et al., 2003).
The flavonoid fraction acts as an antioxidant, scavenging reactive oxygen species and reducing lipid peroxidation in neuronal membranes. In vitro and animal studies have demonstrated neuroprotective effects against amyloid-beta-induced toxicity — relevant to Alzheimer's pathology — but the leap from cell culture to clinical benefit in humans is enormous, and many compounds that look promising in a petri dish fail to deliver in vivo (Bastianetto et al., 2000).
Bilobalide appears to modulate GABA-A receptor activity and may have anti-apoptotic properties in neuronal tissue. Some preclinical work suggests effects on mitochondrial function and neuroplasticity, but again, the human data do not yet confirm that these mechanisms produce measurable cognitive outcomes at the doses used in clinical trials.
How Ginkgo Compares to Other Cognitive Botanicals
Ginkgo has more total clinical data than almost any competing botanical, but that volume has not translated into stronger results for healthy adults. Bacopa monnieri, for instance, has a somewhat stronger evidence base for memory consolidation in healthy adults — a 2014 meta-analysis by Kongkeaw et al. found statistically significant improvements in attention and cognitive processing speed after 12 weeks, which is more than ginkgo biloba cognitive research has demonstrated in the same population. Lion's Mane mushroom (Hericium erinaceus) has shown preliminary positive results for mild cognitive impairment in a small Japanese trial (Mori et al., 2009), but its evidence base is far thinner than ginkgo's overall. Panax ginseng is sometimes stacked with ginkgo in nootropic formulations, though the evidence for the combination is largely limited to a few small studies by the same research group. If you are looking to buy ginkgo biloba extract, the honest comparison is that ginkgo has more total research behind it than almost any competitor, but the results for healthy-adult cognition are no more impressive than those for Bacopa monnieri capsules or other adaptogenic botanicals.


An Honest Limitation: What This Extract Cannot Do
We think it is worth being direct about the ceiling here. Ginkgo biloba cognitive research, taken as a whole, does not support the idea that any dose of ginkgo will turn a healthy brain into a noticeably sharper one. The extract is not a substitute for sleep, exercise, or social engagement — all of which have stronger evidence bases for maintaining cognitive function across the lifespan. We stock ginkgo because the evidence for people with existing mild decline is genuinely interesting, and because customers deserve access to well-standardised botanical products. But we would be doing you a disservice if we implied it was a magic pill. If you order ginkgo extract from us, we would rather you come back in three months and say "I think it helped a little" than feel oversold from day one.

Safety Profile and Interactions
Ginkgo is generally well tolerated in clinical trials, with a safety profile comparable to placebo across thousands of participants (DeKosky et al., 2008). The GEM study, with over 3,000 participants followed for a median of six years, reported no significant difference in overall adverse events between ginkgo and placebo groups. The most commonly reported side effects across trials are mild gastrointestinal complaints, headache, and dizziness.

Ginkgo biloba has documented platelet-aggregation-inhibitor activity and may interact with anticoagulant or antiplatelet medication including warfarin, aspirin, clopidogrel, and NSAIDs. Anyone taking blood-thinning medication, scheduled for surgery, or with a bleeding disorder should consult a qualified healthcare professional before use.
The anticoagulant concern is not theoretical. Case reports have documented spontaneous bleeding events — including subdural haematoma and hyphema — in patients taking ginkgo alongside anticoagulant therapy (Rosenblatt & Mindel, 1997). The GEM trial did not find a statistically significant increase in bleeding events overall, but the trial excluded patients on warfarin, so the interaction risk in that specific population remains poorly characterised in formal settings.
Ginkgo may also interact with anticonvulsant medications by lowering the seizure threshold — a concern raised by case reports rather than controlled studies, but worth flagging for anyone with epilepsy or taking medications like valproate or carbamazepine (Granger, 2001). Pregnant and breastfeeding individuals should avoid ginkgo due to its antiplatelet effects and insufficient safety data in those populations. The EMCDDA does not classify ginkgo as a substance of concern, but the Beckley Foundation has noted the broader challenge of distinguishing well-researched botanical extracts from poorly standardised products in the supplement marketplace.
Study Quality and Publication Bias
A disproportionate share of positive ginkgo results comes from industry-funded trials, while the largest independent studies were negative (Birks & Grimley Evans, 2009; Zhang et al., 2016). One of the persistent problems in ginkgo biloba cognitive research is the gap between industry-funded trials and independently funded ones. The two largest independent trials (GEM and GuidAge) were negative for their primary endpoints. This does not automatically invalidate the industry-funded work, but it is a pattern that any honest reading of the literature has to acknowledge.
The Cochrane review by Birks and Grimley Evans (2009) explicitly noted that many of the older positive trials used outdated methodologies — small sample sizes, inadequate blinding, and outcome measures that would not pass muster by current CONSORT standards. When the reviewers restricted their analysis to trials with adequate allocation concealment and intention-to-treat analysis, the positive signal weakened considerably.
Publication bias is also a factor. A 2016 funnel-plot analysis within Zhang et al.'s overview of systematic reviews found asymmetry suggestive of missing negative studies — meaning that trials showing no effect may simply not have been published. This is a common problem across supplement research and is not unique to ginkgo, but it means the published literature likely overstates the true effect size.
What the Evidence Adds Up To
The overall evidence indicates that ginkgo extract at 240 mg per day may modestly benefit people with existing cognitive decline but does not reliably improve cognition in healthy adults or prevent dementia (DeKosky et al., 2008; Tan et al., 2015). If you line up the evidence by population and outcome, the picture is reasonably clear:
| Population | Outcome Studied | Evidence Direction | Key Source |
|---|---|---|---|
| Older adults, cognitively healthy | Dementia prevention | No benefit detected | DeKosky et al. (2008); Vellas et al. (2012) |
| Patients with mild cognitive impairment or dementia | Cognitive-scale scores (ADAS-Cog, SKT) | Modest positive signal at 240 mg/day for ≥22 weeks | Tan et al. (2015); Zhang et al. (2016) |
| Healthy younger adults | Memory, attention, executive function | No reliable benefit | Laws et al. (2012) |
| Acute single-dose studies (mixed ages) | Speed of attention | Inconsistent, small effects | Kennedy et al. (2000) |
Ginkgo biloba extract — specifically EGb 761 at 240 mg per day — may offer a small, measurable benefit for people already experiencing cognitive decline. For dementia prevention and for cognitive enhancement in healthy people, the large trials have not found a convincing effect. The pharmacology is genuinely interesting (PAF antagonism, antioxidant activity, cerebral blood-flow modulation), but interesting mechanisms do not always translate into clinical results that matter at the individual level.
None of this makes ginkgo useless or fraudulent — it makes it a botanical with a specific, narrow evidence base that is frequently oversold. The traditional use of ginkgo leaf in Chinese medicine dates back to at least the Ming Dynasty (Li Shizhen's Compendium of Materia Medica, 1578), where it was described primarily for respiratory and cardiovascular complaints rather than cognition. The cognitive framing is largely a product of twentieth-century European phytopharmacology, particularly German research from the 1960s onward. Understanding that history helps calibrate expectations. If you order ginkgo extract, look specifically for products standardised to 24% flavone glycosides and 6% terpene lactones — this is the composition used in virtually all credible clinical trials. You can buy ginkgo biloba extract as Ginkgo biloba tincture or Ginkgo biloba capsules from our catalogue.
This article is consumer education, not medical advice. Traditional and ceremonial uses are described for cultural and historical context. Botanicals can interact with medications and are not a substitute for professional care. If you are pregnant, nursing, taking prescription medication, or managing a health condition, consult a qualified healthcare practitioner before use.
References
- Bastianetto, S., Ramassamy, C., Bhatt Doré, S., Christen, Y., Poirier, J. & Bhatt Bhatt, R. (2000). The Ginkgo biloba extract (EGb 761) protects hippocampal neurons against cell death induced by β-amyloid. European Journal of Neuroscience, 12(6), 1882–1890.
- Birks, J. & Grimley Evans, J. (2009). Ginkgo biloba for cognitive impairment and dementia. Cochrane Database of Systematic Reviews, (1), CD003120.
- Braquet, P. (1987). The ginkgolides: potent platelet-activating factor antagonists isolated from Ginkgo biloba L. Drugs of the Future, 12(7), 643–699.
- DeKosky, S.T., Williamson, J.D., Fitzpatrick, A.L. et al. (2008). Ginkgo biloba for prevention of dementia: a randomized controlled trial. JAMA, 300(19), 2253–2262.
- Granger, A.S. (2001). Ginkgo biloba precipitating epileptic seizures. Age and Ageing, 30(6), 523–525.
- Kennedy, D.O., Scholey, A.B. & Wesnes, K.A. (2000). The dose-dependent cognitive effects of acute administration of Ginkgo biloba to healthy young volunteers. Psychopharmacology, 151(4), 416–423.
- Kongkeaw, C., Dilokthornsakul, P., Thanarangsarit, P., Limpeanchob, N. & Scholfield, C.N. (2014). Meta-analysis of randomized controlled trials on cognitive effects of Bacopa monnieri extract. Journal of Ethnopharmacology, 151(1), 528–535.
- Laws, K.R., Sweetnam, H. & Kondel, T.K. (2012). Is Ginkgo biloba a cognitive enhancer in healthy individuals? A meta-analysis. Human Psychopharmacology, 27(6), 527–533.
- Mori, K., Inatomi, S., Ouchi, K., Azumi, Y. & Tuchida, T. (2009). Improving effects of the mushroom Yamabushitake (Hericium erinaceus) on mild cognitive impairment. Phytotherapy Research, 23(3), 367–372.
- Rosenblatt, M. & Mindel, J. (1997). Spontaneous hyphema associated with ingestion of Ginkgo biloba extract. New England Journal of Medicine, 336(15), 1108.
- Santos, R.F., Galduróz, J.C.F., Barbieri, A., Castiglioni, M.L.V., Ytaya, L.Y. & Bueno, O.F.A. (2003). Cognitive performance, SPECT, and blood viscosity in elderly non-demented people using Ginkgo biloba. Pharmacopsychiatry, 36(4), 127–133.
- Tan, M.S., Yu, J.T., Tan, C.C. et al. (2015). Efficacy and adverse effects of Ginkgo biloba for cognitive impairment and dementia: a systematic review and meta-analysis. Journal of Alzheimer's Disease, 43(2), 589–603.
- Vellas, B., Coley, N., Ousset, P.J. et al. (2012). Long-term use of standardised Ginkgo biloba extract for the prevention of Alzheimer's disease (GuidAge): a randomised placebo-controlled trial. The Lancet Neurology, 11(10), 851–859.
- Zhang, H.F., Huang, L.B., Zhong, Y.B. et al. (2016). An overview of systematic reviews of Ginkgo biloba extracts for mild cognitive impairment and dementia. Frontiers in Aging Neuroscience, 8, 276.
Last updated: April 2026
Frequently Asked Questions
9 questionsDoes ginkgo biloba prevent dementia in healthy older adults?
Is ginkgo biloba effective as a nootropic for younger healthy people?
What is EGb 761 and why does it matter for ginkgo biloba cognitive research?
Can ginkgo biloba interact with blood-thinning medications?
How long does ginkgo need to be taken before any cognitive effect appears?
Is there publication bias in ginkgo biloba research?
How does ginkgo compare to Bacopa monnieri for cognitive support?
What should I look for when I buy ginkgo biloba extract?
Is ginkgo biloba safe to take with anticonvulsant medications?
About this article


Adam Parsons is an external cannabis and psychedelics writer and editor who contributes to Azarius's wiki as both author and reviewer. On the writing side, he authors Azarius's kratom and kanna clusters, drawing on exten
This wiki article was drafted with AI assistance and reviewed by Adam Parsons, External contributor. Editorial oversight by Joshua Askew.
Medical disclaimer. This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before use of any substance.
Last reviewed April 26, 2026