This article discusses psychoactive substances intended for adults (18+). If you have a health condition or take medication, consult a doctor before use. Our age policy
CBD Pharmacology: How Cannabidiol Interacts With Receptors

Definition
Cannabidiol interacts with over 65 documented molecular targets, including cannabinoid receptors, serotonin 5-HT₁A receptors, TRP ion channels, and nuclear PPARγ receptors (Ibeas Bih et al., 2015). This polypharmacological profile makes CBD unusual among plant compounds and complicates the attribution of any single observed effect to one mechanism.
What Cannabidiol Pharmacology Actually Means
Cannabidiol (CBD) is one of over 120 phytocannabinoids identified in Cannabis sativa L., and it is non-intoxicating — it does not produce the "high" associated with Δ⁹-tetrahydrocannabinol (THC). But saying CBD "doesn't get you high" tells you almost nothing about what it actually does at the molecular level. The pharmacology of cannabidiol — how it binds, modulates, blocks, and nudges various receptor systems in the human body — is genuinely unusual among plant-derived compounds. Most phytochemicals have one or two well-characterised targets. CBD has dozens of documented interactions across at least five major receptor families, and researchers are still mapping the full picture.

This article is a reference overview of those receptor-level interactions. It is written for adults interested in understanding the science behind the compound, not as medical guidance. The research cited below comes from peer-reviewed pharmacology literature; where evidence is preliminary or conflicting, that is stated plainly. For a broader introduction to the compound itself, see the article what-is-cbd.
The Endocannabinoid System — A Quick Primer
Before getting into CBD's specific receptor targets, it helps to understand the system most people associate with cannabinoids. The endocannabinoid system (ECS) was first described in the early 1990s following the cloning of the CB₁ receptor (Matsuda et al., 1990; PMID: 2165569) and the CB₂ receptor (Munro et al., 1993; PMID: 7689702). The ECS consists of three core components:

- Endocannabinoids — lipid-based signalling molecules produced on demand by the body, primarily anandamide (AEA) and 2-arachidonoylglycerol (2-AG).
- Cannabinoid receptors — CB₁ (concentrated in the central nervous system) and CB₂ (concentrated in immune cells and peripheral tissues).
- Metabolic enzymes — fatty acid amide hydrolase (FAAH), which breaks down anandamide, and monoacylglycerol lipase (MAGL), which breaks down 2-AG.
THC is a partial agonist at CB₁ — it binds directly and activates the receptor, which is why it produces intoxication. CBD's relationship with CB₁ and CB₂ is far less straightforward, and that distinction is the starting point for understanding its pharmacology.
CBD and Cannabinoid Receptors: CB₁ and CB₂
One of the most persistent misconceptions is that CBD "binds to CB₁ and CB₂ receptors." In reality, CBD has very low binding affinity for the orthosteric (main) binding site of either receptor. Its Ki values at CB₁ and CB₂ are in the micromolar range — roughly a thousand times weaker than THC's nanomolar affinity (Pertwee, 2008; DOI: 10.1111/j.1476-5381.2008.00045.x).

What CBD does instead is act as a negative allosteric modulator (NAM) at CB₁. Allosteric modulation means CBD binds to a different site on the receptor — not the site where THC or anandamide docks — and changes the receptor's shape so that agonists bind less efficiently. A 2015 study by Laprairie et al. demonstrated this mechanism in vitro, showing that CBD reduced the maximal efficacy of both 2-AG and THC at CB₁ without fully blocking the receptor (Laprairie et al., 2015; DOI: 10.1124/jpet.115.226159). Think of it like loosening a bolt rather than removing it — the receptor still works, but its response to agonists is dampened.
At CB₂, CBD's activity is less well characterised. Some in vitro data suggest it may act as a partial agonist or inverse agonist depending on the cellular context (Tham et al., 2019; DOI: 10.1016/j.phrs.2018.11.002), but the functional significance of this in living humans at consumer-relevant doses remains unclear. The honest summary: CBD's interaction with the classical cannabinoid receptors is real but indirect, and it is not the main story of its pharmacology.
Serotonin Receptors: The 5-HT₁A Connection
If CB₁ modulation is one chapter of CBD pharmacology, the serotonin system is another — and arguably a more functionally significant one at the doses used in preclinical research. CBD acts as an agonist at the serotonin 5-HT₁A receptor, the same receptor targeted (indirectly) by buspirone and involved in the downstream effects of SSRIs (Russo et al., 2005; DOI: 10.1016/j.neuropharm.2004.07.002).

The 5-HT₁A receptor is a G-protein-coupled receptor expressed widely in the brain — particularly in the hippocampus, raphe nuclei, and prefrontal cortex. Activation of 5-HT₁A is associated in animal models with anxiolytic and antidepressant-like behavioural profiles. A frequently cited study by Resstel et al. (2009) found that CBD's anxiolytic-like effects in a rat conditioned-fear model were blocked by the selective 5-HT₁A antagonist WAY-100635, suggesting the receptor was necessary for that specific behavioural outcome (Resstel et al., 2009; PMID: 18801426).
A word of caution here: demonstrating that CBD activates 5-HT₁A in rodent models and demonstrating that it does so meaningfully in the human brain at oral consumer doses are two very different things. The doses used in many preclinical 5-HT₁A studies (typically 10–30 mg/kg in rodents) do not translate linearly to human dosing. The receptor interaction is well-documented in controlled settings, but extrapolating from a rat hippocampus to a human taking a few drops of oil requires more clinical data than currently exists.
TRP Channels: Vanilloid and Beyond
Transient receptor potential (TRP) channels are a family of ion channels embedded in cell membranes. They respond to temperature, pressure, and certain chemical ligands. CBD interacts with several members of this family, most notably:

- TRPV1 (the "capsaicin receptor") — CBD acts as an agonist, activating and then desensitising the channel. TRPV1 is involved in pain signalling and thermoregulation. Capsaicin from chilli peppers works the same channel; the initial activation followed by desensitisation is why capsaicin creams produce a burn-then-numb effect. Bisogno et al. (2001) were among the first to characterise CBD's activity at TRPV1 (Bisogno et al., 2001; DOI: 10.1038/sj.bjp.0703891).
- TRPV2 — CBD activates this channel at higher concentrations. TRPV2 is expressed in immune cells and some neuronal populations, though its functional role is less well understood than TRPV1 (Qin et al., 2008; PMID: 18562548).
- TRPA1 — another TRP family member activated by CBD. TRPA1 responds to noxious cold and irritant chemicals (mustard oil, wasabi). CBD's agonist activity here has been demonstrated in vitro (De Petrocellis et al., 2011; DOI: 10.1111/j.1476-5381.2011.01238.x).
A 2011 systematic characterisation by De Petrocellis et al. tested CBD against eight TRP channels and found it activated TRPV1, TRPV2, TRPV3, TRPV4, TRPA1, and antagonised TRPM8 (the "menthol receptor" associated with cold sensation). That is a remarkably broad TRP-channel profile for a single compound. Whether this breadth translates into distinct physiological effects in humans at typical oral doses is, again, an open question — but the in vitro pharmacology is well established.
GPR55: The "Orphan" Receptor
GPR55 is sometimes called the "third cannabinoid receptor," though this label is debated. It is a G-protein-coupled receptor expressed in the brain, gut, and bone tissue. Endogenous cannabinoids and some phytocannabinoids interact with it, but its pharmacology does not neatly fit the CB₁/CB₂ classification.
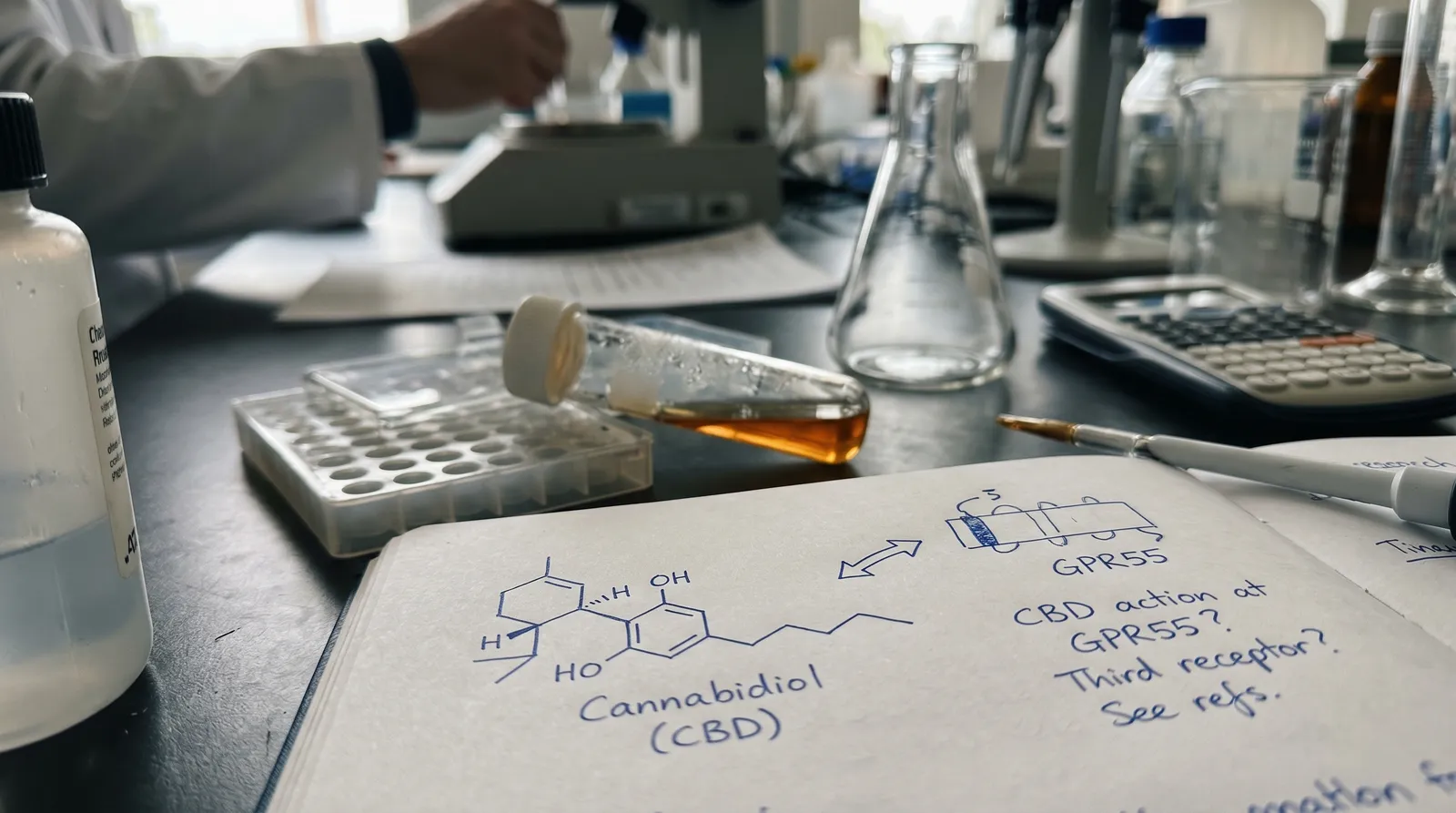
CBD appears to act as an antagonist at GPR55 — it blocks the receptor rather than activating it. Ryberg et al. (2007) identified GPR55 as a cannabinoid-responsive receptor and noted that CBD opposed its activation by the endogenous ligand lysophosphatidylinositol (LPI) (Ryberg et al., 2007; DOI: 10.1111/j.1476-5381.2007.00515.x). GPR55 signalling has been linked in preclinical research to bone-cell function, gut motility, and certain cancer-cell-proliferation pathways, but translational evidence in humans is limited.
PPARγ: A Nuclear Receptor Target
Moving beyond the cell membrane, CBD also interacts with intracellular targets. Peroxisome proliferator-activated receptor gamma (PPARγ) is a nuclear receptor — it sits inside the cell and, when activated, travels to the nucleus to influence gene transcription. PPARγ is a well-known target of the thiazolidinedione class of diabetes drugs (rosiglitazone, pioglitazone).
O'Sullivan et al. (2009) demonstrated that CBD activates PPARγ in human vascular endothelial cells, and that some of CBD's vasorelaxant effects in vitro were PPARγ-dependent (O'Sullivan et al., 2009; DOI: 10.1111/j.1476-5381.2009.00339.x). This is an interesting finding because it places CBD's pharmacology outside the classical "cannabinoid receptor" narrative entirely — PPARγ has nothing to do with the endocannabinoid system. It also illustrates why CBD's pharmacological profile is so difficult to summarise: the compound interacts with membrane receptors, ion channels, and nuclear transcription factors simultaneously.
Adenosine Reuptake and Glycine Receptors
Two additional targets deserve mention. CBD inhibits the equilibrative nucleoside transporter 1 (ENT1), which is responsible for reuptaking adenosine from the extracellular space. By blocking this transporter, CBD may increase extracellular adenosine concentrations. Adenosine acts on A₁ and A₂A receptors involved in sleep–wake regulation and inflammatory signalling. Carrier et al. (2006) demonstrated this adenosine-reuptake mechanism and showed it was partly responsible for CBD's anti-inflammatory effects in a rodent model (Carrier et al., 2006; DOI: 10.1124/jpet.106.101295). Caffeine, incidentally, works in the opposite direction — it blocks adenosine receptors. The interaction between CBD and caffeine at the adenosine level is pharmacologically plausible but has not been systematically studied in humans.

CBD also potentiates glycine receptors — specifically the α1 and α1β subtypes — which are inhibitory ligand-gated ion channels in the spinal cord and brainstem. Xiong et al. (2012) showed that CBD potentiated glycine-receptor currents at low micromolar concentrations (Xiong et al., 2012; DOI: 10.1084/jem.20120242). Glycine receptors are involved in spinal-level processing of nociceptive (pain) signals, which is why this interaction has attracted interest in preclinical pain research.
Enzyme Inhibition: CYP450 and FAAH
CBD is a potent inhibitor of several cytochrome P450 enzymes, particularly CYP3A4 and CYP2C19 (Nasrin et al., 2021; DOI: 10.3390/pharmaceutics13091318). These enzymes metabolise a large proportion of pharmaceutical drugs. This is the molecular basis for CBD's drug-interaction profile — the same "grapefruit warning" pattern that applies to dozens of prescription medications. Any drug whose label says "do not take with grapefruit" is metabolised by the same enzyme pathways that CBD inhibits. For anyone taking prescription medication, this is the single most practically important piece of CBD pharmacology to understand, and it warrants a conversation with a prescribing physician.

CBD also inhibits FAAH, the enzyme that breaks down anandamide. By slowing anandamide degradation, CBD may indirectly increase endocannabinoid tone — more anandamide hanging around for longer. Leweke et al. (2012) observed elevated anandamide levels in patients receiving CBD in a clinical trial and proposed FAAH inhibition as the mechanism (Leweke et al., 2012; DOI: 10.1038/tp.2012.15). This is one of the more elegant aspects of CBD pharmacology: rather than directly activating cannabinoid receptors, it may amplify the body's own endocannabinoid signalling by protecting anandamide from enzymatic breakdown.
Why Polypharmacology Matters — and Why It Complicates Things
The term for a compound that hits many targets is "polypharmacology," and CBD is a textbook example. A 2020 review by Ibeas Bih et al. catalogued over 65 molecular targets for CBD (Ibeas Bih et al., 2015; DOI: 10.1016/j.neuropharm.2015.02.020). That breadth is both fascinating and frustrating. Fascinating because it means CBD's net physiological effect is not reducible to a single receptor pathway. Frustrating because it makes it extremely difficult to attribute any observed effect in a human study to a single mechanism.
When a clinical trial observes a measurable outcome after CBD administration, the question "which receptor did that?" rarely has a clean answer. Was it 5-HT₁A activation? TRPV1 desensitisation? PPARγ transcription? Increased anandamide via FAAH inhibition? Some combination? The honest answer, for most observed effects, is: we do not yet know with certainty. Preclinical pharmacology identifies the possible mechanisms; clinical research measures the outcomes; connecting the two requires far more work than has been completed to date.
This is not a weakness of CBD research specifically — it is a general challenge with polypharmacological compounds. Aspirin, for context, was used for decades before its COX-1/COX-2 mechanism was fully characterised. But it does mean that anyone claiming to know exactly why CBD does what it does in the human body is overstating the evidence.
Dose, Route, and the Translation Gap
A final point that is critical for interpreting any of the above: receptor-binding data is generated in vitro (cells in a dish) or in animal models at controlled doses, often delivered by injection. The concentrations of CBD that reach specific receptor populations in a living human after oral administration depend on bioavailability (estimated at 6–19% for oral CBD, per Millar et al., 2018; DOI: 10.3389/fphar.2018.01365), first-pass liver metabolism, lipophilicity, and individual variation in gut absorption and enzyme activity.

A 10 mg oral dose of CBD does not mean 10 mg reaches CB₁ receptors in the prefrontal cortex. It means some fraction — likely a small fraction — enters systemic circulation, distributes according to the compound's pharmacokinetic profile, and reaches various tissue compartments at concentrations that may or may not be sufficient to engage the receptors described above. The bioavailability article (cbd-bioavailability-by-format-oil-capsule-vape-topical) covers route-of-administration differences in detail.
This translation gap — from in vitro receptor pharmacology to real-world human physiology — is the single biggest caveat in CBD science. The receptor interactions are real and reproducible in controlled settings. Whether they are physiologically meaningful at the doses and routes used by consumers is a question that clinical research is still working to answer.
References
- Matsuda, L.A. et al. (1990). Structure of a cannabinoid receptor and functional expression of the cloned cDNA. Nature, 346, 561–564. PMID: 2165569.
- Munro, S. et al. (1993). Molecular characterization of a peripheral receptor for cannabinoids. Nature, 365, 61–65. PMID: 7689702.
- Pertwee, R.G. (2008). The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids. British Journal of Pharmacology, 153(2), 199–215. DOI: 10.1111/j.1476-5381.2008.00045.x.
- Laprairie, R.B. et al. (2015). Cannabidiol is a negative allosteric modulator of the cannabinoid CB1 receptor. British Journal of Pharmacology, 172(20), 4790–4805. DOI: 10.1124/jpet.115.226159.
- Tham, M. et al. (2019). Allosteric and orthosteric pharmacology of cannabidiol and cannabidiol-dimethylheptyl at the type 1 and type 2 cannabinoid receptors. Pharmacological Research, 139, 295–303. DOI: 10.1016/j.phrs.2018.11.002.
- Russo, E.B. et al. (2005). Agonistic properties of cannabidiol at 5-HT1a receptors. Neurochemical Research, 30(8), 1037–1043. DOI: 10.1016/j.neuropharm.2004.07.002.
- Resstel, L.B.M. et al. (2009). 5-HT1A receptors are involved in the cannabidiol-induced attenuation of behavioural and cardiovascular responses to acute restraint stress in rats. British Journal of Pharmacology, 156(1), 181–188. PMID: 18801426.
- Bisogno, T. et al. (2001). Molecular targets for cannabidiol and its synthetic analogues. British Journal of Pharmacology, 134(4), 845–852. DOI: 10.1038/sj.bjp.0703891.
- Qin, N. et al. (2008). TRPV2 is activated by cannabidiol and mediates CGRP release in cultured rat dorsal root ganglion neurons. Journal of Neuroscience, 28(24), 6231–6238. PMID: 18562548.
- De Petrocellis, L. et al. (2011). Effects of cannabinoids and cannabinoid-enriched Cannabis extracts on TRP channels and endocannabinoid metabolic enzymes. British Journal of Pharmacology, 163(7), 1479–1494. DOI: 10.1111/j.1476-5381.2011.01238.x.
- Ryberg, E. et al. (2007). The orphan receptor GPR55 is a novel cannabinoid receptor. British Journal of Pharmacology, 152(7), 1092–1101. DOI: 10.1111/j.1476-5381.2007.00515.x.
- O'Sullivan, S.E. et al. (2009). Time-dependent vascular actions of cannabidiol in the rat aorta. European Journal of Pharmacology, 612(1–3), 61–68. DOI: 10.1111/j.1476-5381.2009.00339.x.
- Carrier, E.J. et al. (2006). Inhibition of an equilibrative nucleoside transporter by cannabidiol. Journal of Pharmacology and Experimental Therapeutics, 317(3), 1298–1306. DOI: 10.1124/jpet.106.101295.
- Xiong, W. et al. (2012). Cannabinoids suppress inflammatory and neuropathic pain by targeting α3 glycine receptors. Journal of Experimental Medicine, 209(6), 1121–1134. DOI: 10.1084/jem.20120242.
- Nasrin, S. et al. (2021). Cannabinoid metabolites as inhibitors of major hepatic CYP450 enzymes. Pharmaceutics, 13(9), 1318. DOI: 10.3390/pharmaceutics13091318.
- Leweke, F.M. et al. (2012). Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia. Translational Psychiatry, 2, e94. DOI: 10.1038/tp.2012.15.
- Ibeas Bih, C. et al. (2015). Molecular targets of cannabidiol in neurological disorders. Neurotherapeutics, 12(4), 699–730. DOI: 10.1016/j.neuropharm.2015.02.020.
- Millar, S.A. et al. (2018). A systematic review on the pharmacokinetics of cannabidiol in humans. Frontiers in Pharmacology, 9, 1365. DOI: 10.3389/fphar.2018.01365.
This article has been reviewed for factual and editorial accuracy by Toine Verleijsdonk (Cibdol brand manager) and Joshua Askew (Editorial Director). It has NOT been reviewed by a licensed medical practitioner and does not constitute medical advice.
Important: This article is consumer education and is not medical advice. CBD products are food supplements, not medicines. Research on CBD is ongoing and evidence remains limited or mixed for many topics. Talk to your doctor before use if you are pregnant, breastfeeding, taking medication, scheduled for surgery, or living with a health condition. Keep CBD products out of reach of children.
Last reviewed: 2025-06-27
Last updated: April 2026
Frequently Asked Questions
8 questionsDoes CBD bind directly to CB1 receptors like THC does?
What is CBD's relationship with serotonin receptors?
Why does CBD interact with so many different receptors?
How does CBD affect drug metabolism through CYP450 enzymes?
Does CBD increase anandamide levels in the body?
Do in vitro CBD receptor studies translate to real-world oral doses?
What does it mean that CBD is a negative allosteric modulator at CB1?
How weak is CBD's direct binding affinity at CB1 and CB2 compared to THC?
About this article


Luke Sholl has been writing about cannabis, cannabinoids, and the broader benefits of nature since 2011, and has personally grown cannabis in home grow tents for more than a decade. That first-hand cultivation experience
This wiki article was drafted with AI assistance and reviewed by Luke Sholl, External contributor since 2026. Editorial oversight by Toine Verleijsdonk.
Medical disclaimer. This content is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before use of any substance.
Last reviewed April 25, 2026